Contents
Foreword
Schools have an important role to play in supporting mental health and wellbeing… by developing approaches tailored to the particular needs of their pupils.
The culture, ethos and environment of the school can have a profound influence on both pupil and staff mental wellbeing. Environments that are hostile, aggressive, chaotic or unpredictable can be harmful to mental health, and can lead to stressful teaching and working conditions. Schools are in a unique position, as they are able to help prevent mental health problems by promoting resilience as part of an integrated, whole school approach that is tailored to the needs of their pupils. DfE (2018) Mental Health and Behaviour in Schools.
Purpose of this document
The Educational Psychology Service and SEMH Advisory Team have produced guidance for schools and settings on supporting the emotional health and wellbeing of staff and pupils. Research indicates a growing number of young people are experiencing mental health difficulties, particularly following the Covid-19 pandemic. There is now a greater need for senior leaders to review their settings’ approach to emotional health and wellbeing.
This document provides evidence-based guidance for education settings and providers on ways to effectively support the emotional health and wellbeing of staff and pupils. It is structured around a 7 Factor Model for effective emotional health and wellbeing underpinned by research, and signposts schools to resources and support from local and national organisations.
If you have any questions about this document, please contact Dr Daniel Nicholls, Senior Educational Psychologist
Dan.nicholls@devon.gov.uk
How can schools use this document?
This document can be used by School Governors, Senior Leaders, Special Educational Need Coordinators and Pastoral staff to:
- Understand the current local and national context around emotional health and wellbeing.
- Identify areas of strength and weakness within current provision for the emotional health and wellbeing of staff and pupils which can feed into targeted CPD and school action plans.
- Develop and embed an ‘assess, plan, do, review’ process for students with emotional health and wellbeing needs and identify resources to understand and assess need.
- Identify evidence-based assessments and interventions to support emotional health and wellbeing.
- Understand a graduated response to emotional health and wellbeing e.g. universal, targeted and specialist support, including when referrals need to be made to other agencies.
- Clarify support from and signpost to local and national organisations.
Considerations for School Governors, Senior Leaders, SEN and Pastoral staff are in bold and italics for ease of access.
A ‘Jargon Buster’ defining key terminology can be found in Section 14.
1. Introduction
1.1. Definitions of Emotional Health and Wellbeing (EHWB)
The terms emotional health, wellbeing and mental health are all used interchangeably and refer to your mental state: how you are feeling and how well you can cope with day-to-day life.
Our mental wellbeing is dynamic. It can change from moment to moment, day to day, month to month, year to year. If you have good mental wellbeing, you are able to:
- Feel relatively confident in yourself and have positive self esteem
- Feel and express a range of emotions
- Build and maintain good relationships with others
- Feel engaged with the world around you
- Live and work productively
- Cope with the stresses of daily life
- Adapt and manage in times of change and uncertainty
The World Health Organisation (WHO) defines mental health as:
a state of wellbeing in which every individual realizes his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully. (WHO, 2014).
Sustainable wellbeing includes the experience of functioning well, for instance having a sense of engagement and competence, being resilient in the face of setbacks, having good relationships with others and a sense of belonging and contributing to a community. (Huppert 2013).
We are all different. What affects someone’s mental wellbeing won’t necessarily affect others in the same way. (Mind 2016).
1.2. The difference between EHWB and Mental Health problems
Short term stress and worry is a normal part of life and many issues can be experienced as mild or transitory challenges for some children and their families. Others will experience more serious and longer lasting effects. The same experience can have different effects on different children depending on other factors in their life. For example, it is normal for children to feel nervous or under stress around exam times, but other factors can make such stress part of an enduring and persistent mental health problem.
When a problem is particularly severe or persistent over time, or when a number of these difficulties are experienced at the same time, children are often described as experiencing mental health problems.’ (DFE 2018). These problems have a significant impact on daily functioning.
Mental health problems in children and young people may be categorised under the following headings:
Anxiety
Anxiety is a natural human response, it is what we feel when we are worried, tense or afraid and is particularly common while coping with stressful life events or changes. Anxiety can become a mental health problem if it impacts on your ability to live your life as fully as you want to.
Borderline Personality Disorder
This is disorder of mood and how a person interacts with others, generally someone with a personality disorder will differ significantly from an average person in terms of how they think, perceive, feel or relate to others.
Depression
Depression is a common but serious mood disorder that causes persistent feelings of sadness and loss of interest. It can impact on the ability to complete day to day activities and can lead to a variety of physical and emotional problems.
Eating Disorders
A difficult relationship with food which impacts on your mental health. This is a medical diagnosis which is made based on eating patterns and medical tests on weight, blood, and body mass index (BMI).
Obsessive Compulsive Disorder
Obsessions are unwelcome thoughts, worries or urges that repeatedly appear in your mind, and compulsions are the repetitive activities you do to reduce anxiety caused by the obsession.
Post-traumatic Stress Disorder
Post-traumatic stress disorder (PTSD) may develop as a result of an acute stress reaction after being involved in, or witnessing, traumatic events. People with PTSD often re-live the traumatic event through nightmares and flashbacks. They may have problems sleeping and concentrating. These symptoms are often severe and persistent enough to have a significant impact on the person’s day-to-day life.
Psychosis
Psychosis is described as perceiving or interpreting reality in a very different way from people around you, characterised by delusions and / or hallucinations.
Schizophrenia
Schizophrenia is a medical diagnosis described as a severe long-term mental health condition where the person may not always be able to distinguish their own thoughts and ideas from reality.
Further information can be found at:
If a child or young person is experiencing a mental health problem, it is crucial that schools seek advice and support from specialist mental health services such as CAMHS, however, staff can continue to support these young people by promoting good emotional health and wellbeing within the education setting and by fostering supportive and nurturing relationships with the children and young people in their care.
The Emotional Health and Wellbeing Pathway in Section 11.1 can be used by schools and settings to determine the level of need a pupil is presenting with, and to identify the type of support required.
1.3. The impact of EHWB on educational outcomes and life chances
The impact of poor emotional health and wellbeing on children and young people’s educational outcomes and life changes is well documented.
In 2019, the Head Start Project funded by the National Lottery Community Fund conducted a research study into emotional health and wellbeing in schools in partnership with the Evidence Based Practice Unit (EBPU) at University College London (Lereya, T., & Deighton, J. 2019).
Over 15,000 Year 7 pupils from England completed questions about their mental health and the research found that:
- Young people with identified mental health needs were more likely to have lower attainment levels and be persistently absent from schools (persistent absence means that pupils missed 10% or more of lessons).
- Persistent absence was higher for young people with emotional difficulties, behavioural difficulties and hyperactivity or attention difficulties.
- Young people who were excluded from schools, had higher scores for behavioural difficulties, difficulties with peers and attention difficulties.
- Those who were excluded from school, had lower scores for emotional strengths and skills, positive wellbeing and support networks.
Lead author, Dr Tanya Lereya, said:
The results of the current study highlight the importance of prevention, early intervention and school-based support for mental health difficulties and the importance of integration between mental health support and policy creation in relation to mental health difficulties and wellbeing in schools.
Exclusion data from the Department for Education (DfE, 2018a) indicates that the level of permanent exclusions from school remained relatively stable at 0.10% between 2016/17 to 2017/18, which is the equivalent of 10 students per 1000. However, the number of fixed term exclusions has increased in primary and secondary schools with 14% of excluded students being eligible for Free Schools Meals, 43% being identified as having SEND, and Gypsy/Roma and travellers of Irish Heritage ethnic groups having the higher fixed term exclusion rates.
If young people who have been excluded from school, do have poorer EHWB, as found by the Head Start Project, the DfE data highlight that whilst universal support to improve young people’s EHWB is needed, vulnerable groups may require additional, targeted support.
In addition to the link between poor EHWB and poor educational outcomes, there are a myriad of are further concerns about the wellbeing of our children and young people in modern society.
The Good Childhood Report (2019) found that while most children enjoy their childhood, young people are less happy now; with issues such as boys’ appearance, friendships and school identified as potential driving factors. Children struggle as a result of their family finances and worry about what their future might be like. Additionally, they have increasing concerns around crime, climate change and the dangers of technology.
To add to this picture:
- Over the past 20 years, the prevalence of mental disorders in children and young people aged 5 to 15 has increased from 9.7% to 11.2% (NHS, 2018).
- There are concerns about the impact of social media on wellbeing, including concerns about bullying and negative body image.
- There are widely published safeguarding concerns linked to county lines, radicalisation, gang/criminal activity and childhood exploitation.
- We remain in a climate of austerity whereby support services and resources may be limited and there have been additional significant and complex stressors due to the COVID 19 pandemic.
1.4. National guidance to support EHWB
Supporting children and young people’s EHWB is high on the national agenda and increasingly schools are being asked to play a key role in this which has been reinforced in a number of reports and guidance documents in recent years:
Future in Mind: Promoting, protecting and improving our children and young people’s mental health and wellbeing: The Department of Health set out its aspiration that by 2020 professionals working with children and young people will be ‘trained in child development and mental health, and understand what can be done to provide help and support for those who need it’ (Department of Health & NHS England, 2015).
Five Year Forward: In 2016, NHS England set out the current state of mental health service provision in England and made recommendations in all service areas to improve services for children and young people including a focus on mental health.
Transforming Children and Young People’s Mental Health Provision (Department of Health & Department of Education, 2017). This green paper outlines proposals for every school to have a designated senior lead for mental health. Additionally, they propose that mental health support teams will be created to support groups of schools and colleges, offering individual and group intervention to young people with mild to moderate mental health difficulties. These teams will work alongside designated mental health links and provide a connection to specialist services. This approach is currently being rolled out in Devon.
Supporting Mental Health in Schools and Colleges (Department for Education, 2017). This research highlights what schools, colleges and other educational institutions in England currently do to promote wellbeing amongst their pupils, how they identify and support pupils who might have particular mental health needs or require specialist support, and what their experiences are of putting this provision into place.
Mental Health and Behaviour in Schools (Department for Education, 2018). This guidance outlines expectations for schools to support children and young people’s mental health. It encourages schools to consider their culture and ethos and how they support the wellbeing of staff. It sets out expectations that school staff are trained in mental health and describes how to identify and support young people experiencing difficulties. It also states that all schools should identify a Lead for Mental Health.
Social and Emotional Wellbeing in Primary and Secondary Education draft scope for consultation (National Institute for Health and Care Excellence, 2019). NICE are currently updating their guidance for schools on evidence based approaches to support social and emotional wellbeing. This is due to be published in 2021.
The Ofsted Common Inspection Framework (2019). The new Ofsted Framework has a key focus on children’s emotional health and wellbeing and the wellbeing of school staff. Areas of focus includes Personal Development and Behaviour and Attitudes.
The Government is making relationships education compulsory for all primary pupils. Relationships and Sex Education (RSE) is compulsory for secondary pupils and Health Education is compulsory for all pupils in all primary and secondary state-funded schools. This includes a requirement for pupils to learn about mental health and wellbeing (DfE, 2019). This will be compulsory from September 2020.
2. The local context in Devon
2.1. Devon data and local needs
Devon reflects the national picture in regards to concerns about the EHWB of children and young people, however, there are also some specific needs identified within the county.
As part of the Government initiative, Five Year Forward View for Mental Health (2016), NHS England set targets for Clinical Commissioning Groups to achieve by 2020 and ‘Transformation Plans’ for improving access to services were put in place in all Local authorities.
In January 2018, the Sustainability and Transformation Partnership (STP) which covers Devon, Plymouth and Torbay, highlighted the following:
- The STP has a higher proportion of children identified with social, emotional and mental health needs as their primary SEN, than the national average.
- There has been an increase in admissions for self-harm amongst 10-24 year olds; the rise is most marked amongst 10-14 year olds and 15-19 year olds. Rates are higher than the national average across the whole STP.
- Children in Care across the STP have higher levels of emotional and behavioural difficulties than average.
These findings highlight the importance of prevention and early intervention to improve the emotional health and wellbeing of children and young people in Devon.
3. The impact of the COVID 19 pandemic on emotional health and wellbeing in schools
The onset of the COVID 19 pandemic and social distancing measures brought additional and particular challenges to schools and educational settings in supporting wellbeing of students and staff. Early evidence indicated a significant impact on children and young people’s wellbeing. Young Minds carried out a survey of 2111 young people with lived experience of mental health problems to find out how the pandemic and lockdown were affecting them. Results of the survey indicate that 83% of young people said the pandemic had made their mental health ‘a bit’ or ‘much’ worse. Many young people reported missing face to face support although 74% said that they were still able to access mental health support remotely. Additional concerns related to their family’s health, a loss of routine, loss of social connection and worries over school and university closures.
As we emerge from the pandemic, there is a growing body of research related to its impact on the emotional health and wellbeing of children and young people. Whilst complex and variable for individuals, data suggests a general increase in wellbeing difficulties for children and young people in England during the pandemic (NHS, 2021). Those with existing mental health needs or other vulnerability indicators such as SEN or economic disadvantage have been found to have experienced more significant and persistent difficulties following the pandemic.
State of the nation 2021: children and young people’s wellbeing – GOV.UK (www.gov.uk)
There is also increasing attention being given to the impact of Long Covid on children and young people’s health and education. Research indicates that Long Covid can increase feelings of anxiety and depression, whilst also affecting important cognitive functions such as attention and memory. It will be important for schools and educational settings to understand and meet the needs of children and young people experiencing Long Covid.
Links to research and resources for parents, schools and educational settings can be found here:
Further information regarding Long Covid can be found here:
Long-term effects of coronavirus (long COVID) – NHS (www.nhs.uk)
Reports from Early Help and MASH both locally and nationally suggest an increase in Domestic Abuse and Neglect during the COVID 19 pandemic. The Devon Safeguarding Children Partnership can provide further advice and support:
4. The role of schools in supporting emotional health and wellbeing
Schools have a significant role to play in supporting the emotional health and wellbeing of students. National policy and guidance recognises the importance of whole school approaches to wellbeing for all (universal provision), alongside targeted intervention and provision for ‘at risk’ groups and pupils showing early signs of difficulty.
Professor Katherine Weare undertook a systemic review of the literature in this area in 2015 and found that the research indicates that there are seven key factors that schools should consider if emotional health and wellbeing is to be addressed effectively. These are:
1. Adopt whole school thinking:
- Use a ‘whole school approach’.
- Have a solid base of positive universal provision to promote wellbeing.
- Develop a supportive school and classroom ethos which builds a sense of connectedness, the acceptance of emotion and vulnerability, warm relationships and the celebration of difference.
- Start early with skills-based programmes, preventive work, the identification of difficulties and targeted interventions.
- Promote staff wellbeing, and in particular address staff stress.
2. Engage the whole community
- Engage pupils through encouraging pupil voice, authentic involvement in learning, decision-making, and peer-led approaches.
- Engage parents/carers and families in genuine participation, particularly those of pupils in difficulties whose families may feel blamed and stigmatised.
3. Prioritise professional learning and development
- Understand and reduce the risk factors that can affect wellbeing, and help pupils develop the resilience to overcome adverse circumstances.
- Raise staff awareness about mental health problems in children and the school’s responsibility to identify them and intervene early.
- Base their response on a sound understanding of child and adolescent development.
- Help all pupils cope with predictable life changes and transitions. Keep abreast of new challenges posed by information technology, such as cyber bullying.
4. Implement targeted programmes and intervention
- Ensure high-quality implementation of specific programmes and interventions.
- Explicitly teach social and emotional skills, attitudes and values, using well trained and enthusiastic teachers and positive, experiential and interactive methods and resources.
5. Develop supportive policy
- Ensure that there are robust policies and practice in key areas such as behaviour, anti-bullying and diversity, including tackling prejudice and stigma around mental health.
6. Link EHWB to behaviour management approaches
- Respond thoughtfully to challenging behaviour, both responding actively with clear consequences but also seeking to understand its deeper roots, taking opportunities to model and teach positive alternatives.
7. Implement targeted responses and identify specialist pathways
- Provide more targeted and intense work on social and emotional skill development for pupils experiencing difficulties individually or in groups.
- Use specialist staff to initiate innovative and specialist programmes transferring responsibility to mainstream staff whenever possible, to ensure longer term sustainability and integration.
- Where pupils experience difficulties, provide clear plans and pathways for help and referral, using a coherent teamwork approach, including outside agencies such as CAMHS.
(The above is taken from, National Children’s Bureau School Wellbeing Framework Leaders Resources; referenced below.)
The National Childrens Bureau has produced a Whole School Framework of Emotional Wellbeing and Mental Health which brings together research evidence to support schools to create an effective and sustainable approach to promote and respond to the emotional health and wellbeing needs of both students and staff.
Whole school approach (ncb.org.uk)
You may wish you use this self-assessment tool to identify strengths and areas for development in your setting.
NCB School Well Being Framework Leaders Tool FINAL.pdf
Sections 5 – 11 of this document use Katherine Weare’s (2015) Seven Factor Model to outline in more detail how schools and settings can effectively promote emotional health and wellbeing for staff and pupils within the Devon context signposting to evidence-based resources and local support services.
5. Adopt whole school thinking
The DfE (2018) emphasize the need for schools to use “a consistent whole school approach” to support children’s wellbeing and mental health. Additionally, in the 2015 report from the Children and Young People’s Mental Health and Wellbeing Taskforce (DoH & NHS England, 2015) it is identified that there is a national commitment to the development of whole school approaches to promoting mental health and wellbeing. As such, it is vital that schools and education settings continuously look for opportunities to embed practice and reinforce the message of positive emotional wellbeing within the whole school community, throughout the building, in lessons, during assemblies, amongst staff and pupils, through social activities and school trips, with parents, at break and lunch times, through breakfast clubs and after school clubs and out into the wider community.
Resources are available to help schools develop whole school approaches to emotional wellbeing via:
- https://www.mentallyhealthyschools.org.uk/
- https://www.emotionallyfriendly.co.uk/
- Sandwell Wellbeing Charter Mark
- Devon Educational Psychology Service can provide training and leadership support to develop and implement whole school Relational Approaches and Practice.
5.1. The psychology of emotional health and wellbeing
In order to create a whole school ethos that promotes positive EHWB, staff need to have an understanding of the psychology of wellbeing. There are numerous psychological theories of emotional health and wellbeing. An understanding of these theories and approaches can be useful for school staff as they underpin whole school approaches to EHWB and evidenced-based interventions. It may be useful to consider providing staff with CPD in this area.
Positive psychology
Positive psychology can be described as the scientific study of what constitutes an engaged and meaningful life. Positive psychology is studied in order to learn how best to help people to best enjoy their lives. The approach focuses on strengths rather than weaknesses, studying thoughts, feelings and behaviour such as life satisfaction, self-esteem, hope and gratitude (Peterson, C. 2009).
There are three pillars of positive psychology;
- Positive experiences: for example, happiness and love
- Positive individual traits: for example, resilience and compassion
- Positive institutions: for example, applying the principles within organisations
The PERMA model is one model that is used to understand wellbeing in greater depth. It identifies 5 essential elements to wellbeing;
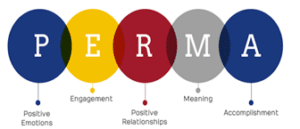
P – Positive emotion
E – Engagement
R – Relationships (positive)
M – Meaning
A – Accomplishment or Achievement
These five aspects of the PERMA model can provide a framework to understand wellbeing and as a foundation for improving wellbeing (Seligman, M. 2011).
(Image retrieved from: https://positivepsychology.com/what-is-positive-psychology-definition/#references)
Resilience
Resilience can be defined as successful adaptation to challenging circumstances, overcoming stress and adversity. Resilience can help to explain the fact that people respond differently to trauma and stress.
Resilience is not a single factor but involves the interplay of risk and protective factors both within the individual and in their environment including their family and school.
Risk factors can accumulate to make someone more vulnerable to stressors, whereas cumulative resilience factors protect against the negative impact of stressors. The more protective factors that are present, the better chance an individual will be able to adapt positively in challenging circumstances (Masten, A. S., & Barnes, A. (2018).
Resilience factors include:
- Individual factors: self-esteem, emotional regulation, sense of purpose.
- Family factors: positive parenting, low family stress, stability.
- Community factors: supportive extended family, positive school experiences, safe neighbourhood, extracurricular activities (Kumpfer, K. L. (2002).
Attachment
In 1969, John Bowlby described the importance of the attachment relationship between the infant and the primary care giver for the child’s survival and development. Bowlby considered that a ‘good enough’ attachment to the parent provided the infant with a secure base from which to explore and engage with others and their environment. He suggested that early attachments form templates through which the child grows to understand the value of themselves and relationships. The quality and responsiveness of the relationship and in particular, the interactions between the infant and caregiver, dictate whether the infant experiences the relationship as valuable, reliable and safe. In order to gain meaning from the world and to develop socially and emotionally, infants need to develop a secure relationship with at least one primary caregiver (Bowlby, 1969). Recent advances in neuroscience have linked early attachment with brain development (Dunnett and Jones, 2018).
Children at any age can develop secure attachments which enable them to feel safe, secure and good about themselves. Children who are not securely attached at home need a significant adult in school who can provide them with a secondary attachment and become a ‘safe base’ from which they can begin to explore and learn. A secure relationship involves the adult providing high levels of protection, connection, understanding and care. These are the cornerstones of the pupil / teacher relationship. It is through regular and repeated opportunities for the child to feel protected, connected with, understood and cared for that they can feel safe and secure and begin to trust and form secure attachments (Dunnett and Jones, 2018).
5.2. Promoting staff wellbeing
Staff wellbeing and pupil wellbeing are intertwined. Children’s behaviour in school is cited as the leading cause of teacher stress and the main reason for teachers leaving the profession. Teachers often have poor work / life balance and may be dealing with stressful and complex issues on a daily basis.
Actively promoting and supporting teacher wellbeing has been found to have a positive impact on staff performance, morale and retention which in turn has a positive impact on pupil outcomes, attainment and wellbeing (Mentally Healthy Schools – see link below).
The Anna Freud Centre provide advice on supporting the wellbeing of school staff as part of their Mentally Healthy Schools Programme.
The below are essential elements to successfully achieving staff wellbeing and in turn, positive outcomes for all. You may wish to consider how effectively these core elements of staff wellbeing are embedded within your setting.
Developing and embedding core values
By developing strong, shared values across a school, it can increase commitment, create a sense of belonging, and drives motivation as staff actively work together towards the core values. A shared vision that is co-created can collectively excite, engage and encourage behaviours and actions that help to fulfil these core values, especially when they are modelled, reinforced and rewarded across the school community by senior leadership. For core values to be meaningful, they need to be explicit, transparent and visible for all staff to understand what they are working towards and enable the vision to be truly shared among all and embedded throughout the school.
Ensuring staff feel valued, accepted and supported
Staff look to their senior leadership team for guidance, encouragement, and to model how they engage and interact with others. The importance of positive interaction and feedback cannot be underestimated; feedback helps staff to feel valued and supported, makes them more resilient, confident and hard working.
As such, it is important to:
- Ensure that frequent and positive interactions occur between staff members both peer to peer and from the leadership team and to other staff members. Schedule in time to talk with one another formally or informally to provide increased opportunities for these positive interactions.
- Provide positive feedback and recognition. By giving positive feedback, we can increase people’s confidence and make them feel appreciated and valued.
- Show genuine concern and consideration for staff as individuals through demonstrating sensitivity, warmth and respect.
Encouraging a sense of cohesion
As individuals, it is important to our self-identity to have and develop feelings of belongingness to a range of groups including our family, friends and work. To feel part of a group, a sense of security, feelings of being wanted as well as supported are essential, otherwise we may feel and become detached.
“Teams” can easily be created but it is through a group of people working together and having opportunities to socialise together that a team, in its truest sense, which supports and encourages each other is formulated. To support a sense of group and team cohesion, consider the following:
- Nurture an atmosphere of learning and development through positive reflection and support. Provide opportunities for staff to share their experiences and reflections with others such as during staff meetings or in school newsletters.
- Facilitate good working relationships and establish a professional culture by providing protected time for teachers and TAs to meet to discuss lesson plans and interventions, introducing “business breakfasts” for lead subject teachers or heads of years to discuss how they are developing their practice and giving TAs time to meet as group to discuss interventions, strategies and share resources.
- Organise a range of social events that provide fun and enjoyment, building on group cohesion and belonging. Consider a range of activities and the timing of them throughout the school year to enable people of different cultures, and backgrounds to come together without any possible barriers such as childcare or dietary requirements.
Positive working environment
The environment in which we are in can have a positive or negative impact upon the way we feel. Managing busy classrooms and corridors can be undoubtedly stressful so having a protected staffroom space to relax, unburden any difficulties and gain support from your colleagues in is essential for staff wellbeing.
To help create a positive, relaxing staffroom environment, it is important to:
- Consider the staffroom layout and contents, ensuring spaces for communal conversations, added comforting features such as cushions and posters and minimizing work clutter. It should feel like a sociable area, not a storage room or work area.
- Where possible, provide provisions for staff such as readily available tea, coffee and fruit. Spontaneously provide break time treats such as ice cream in summer or mince pies at Christmas, providing a shared enjoyable experience while letting staff know that they are cared for.
- Notice boards within the staffroom can be used to help promote staff wellbeing if kept up to date and clutter free. Use them to communicate to staff about forth coming social events, provide staff messages such as writing positive feedback to one another and celebrate positive events such as birthdays and anniversaries.
Actively supporting staff wellbeing at a universal, targeted and individual level
We all need varying levels of support and consideration at different times in our lives as often unforeseen events occur either at home, in work or both. Sometimes, it can only take one thing to change for us to feel destabilised and require those around us to adjust the way they support us. As such, it is important to think about staff wellbeing at a universal, targeted and individual level.
Universal staff support
- Explicitly let staff know that their wellbeing is important. Provide regular wellbeing slots during staff meetings to provide messages of what is being done to support their wellbeing, do a wellbeing activity or share good news items.
- Provide a staff wellbeing guidance document or policy that staff have all had the chance to contribute to that outlines how the school is looking after their staff.
- Senior leadership team to model and encourage good working practices, self-care and emphasize the importance of a healthy work / life balance. This can be done through leadership team being seen to make drinks in the staff room, take breaks and enjoy lunch with colleagues, asking for help and support from varying staff and leave work on time regularly.
- Where possible, consider if subsidies can be sought for staff to access gym or counselling services as a means to provide staff with further ways to support their wellbeing outside of the workplace, in turn, reducing the amount of time off staff have through stress.
- Provide opportunities (feedback box, ideas board) for staff to give feedback and ideas about how the school ethos and shared values could be further achieved.
- Dedicated work free zones within school.
- Fortnightly before or after school specialist activities that focus on wellbeing such as yoga, mindfulness, having a psychologist come in and talk about managing stress techniques, emotional fitness training, or peer massage. Get staff to contribute their ideas and vary the days and times to allow for people’s varying work patterns.
- Ensure staff are consulted regularly about any proposed changes to the school and communicate clearly with them so that everyone feels equally included.
- Provide all staff with the basic skills to support children and young people’s emotional wellbeing. Where staff feel deskilled, this negatively impacts upon their own wellbeing.
- Organise health and wellbeing days for all staff, providing professional input into how they can increase their own wellbeing while also providing opportunities to engage in wellbeing activities.
Targeted staff support
- Provide additional training around mental health for school staff who have a greater role in supporting individual children with additional emotional wellbeing needs. This could be external training such as First Aid training for Mental Health or through online resources such as https://www.minded.org.uk/
- Supervision with peers, either in school or from a neighbouring school (see supervision section below).
- Regular wellbeing check in meetings with a staff member of their choosing for personal or peer support.
Individual staff support
- Support staff members to access available support services through highlighting employee assistance programmes that they may not be aware of or feel able to access alone.
- Refer individuals to Occupational Health to ensure their needs are fully assessed and to seek advice on appropriate support.
- Allow for flexible working. Sit with the individual and think about potential sources of stress within the school day and how they can be supported through them by either having their duties reduced for certain activities e.g. not having to cover break or lunch time duty or having alternative strategies in place e.g. having additional TA support during a particular lesson.
- Help them to develop skills that may be a particular difficulty such as time management, behaviour management or life/work balance.
- Provide a peer buddy that they can go to at any time about any worries or concerns, being explicit that this will have no implication on performance management processes.
- Enable staff to take “time-out” during the school day and ensure that a work free zone is available to that staff member during this time.
- Education Support is the only UK charity dedicated to improving the health and wellbeing of the education workforce. They have a free helpline run by trained counsellors. https://www.educationsupport.org.uk/
Nurturing staff expertise
As humans, we typically want to do interesting things and seek out opportunities where we can engage in things that we are passionate about. When given the chance, people can do some astounding things as we all typically have an innate drive towards being challenged and have a desire to master something. Where schools can provide opportunities for their staff to explore their passions and develop specialisms, it will give staff a greater sense of purpose and highlight their value as an individual within the school community as well as improving the school’s overall skills and knowledge. This also role models curiosity and challenge in learning to students.
There are many ways to nurture staff expertise in schools, including:
- Getting to know where staff’s strengths and interests currently lie and seeking out opportunities for them to use them within the school e.g. taking the lead on an assembly relating to a topic area of their interest or developing an INSET to staff to share their expertise.
- Create a ‘Specialists Board’ outlining the different interests and specialisms that all staff have and place it where it can be shared with all staff members.
- Foster teachers’ and teaching assistants’ areas of interest by providing time to develop resources, complete further reading or attend training to advance their knowledge in their chosen area.
Supervision
Within the clinical, psychological and counselling arenas, supervision is a core part of professional practice and is an expectation of their working life. It is, therefore, perhaps surprising, that school staff are not regularly provided with the same opportunities. Given its importance in supporting staff wellbeing and in turn, providing better outcomes for children and young people, it is essential that schools consider how appropriate supervision can be embedding into schools, particularly for those staff members who are working with children and young people with significant SEMH difficulties such as pastoral leads and attachment-based mentors.
Supervision should be delivered by a professional with training in supervisory skills, who also has expertise and experience of children and young people with difficulties in this area. Where this is not available, alternative models of peer and group supervision could be sought internally within schools such as using a solution circle. It is important for supervision to be separate from any form of performance management and therefore not carried out with individual line managers where possible.
The Devon Educational Psychology Service and SEMH Team can provide clinical supervision for school staff. Please discuss with your link practitioner.
6. Engage the whole community
6.1. Promoting pupil voice
In order for settings to truly and effectively promote positive EHWB they need to genuinely seek the views of pupils and work closely with parents and carers.
While the right for children and young people to have their voices heard is well known through the United Nations Convention on the Rights of the Child (UNCRC, 1989), it is essential to recognise the importance of this right and to consider the impact that gaining and listening to pupil’s voices has on their emotional wellbeing. As the recipient of school services, children and young people can provide a unique perspective.
Pupil voice refers to children and young people’s participation, contribution and influence within a school or education setting (MacBeath, 2006). It is recognised that by involving children and young people in decisions that affect them, they benefit through improved health and wellbeing, improved engagement and behaviour, and improvements in learning, achievements and school performance (Pupil participation: a best practice guide, 2016).
In order to truly gain pupil’s voice, it is important to consider the following:
- When is the best time? Do you have enough time to ensure that the child feels truly listened to?
- Where might be the best place to obtain their views? During a whole class activity or PHSE lessons to gain a wide range of views, through small group work or in 1:1 activities?
- Who is the best person to get the pupil’s voice? Is there an adult that the child trusts well and feels able to speak freely with?
- Are the child’s views going to be confidential or widely known? This may impact upon their perception of whether they can freely provide their views.
- What resources will be used to get the pupil’s views? A whole school approach may take a school survey approach such as using the Pupil Attitude to Self and School (PASS), Pupil and Staff Wellbeing Measure or an individualised approach using sorting cards (The Therapeutic Treasure Deck of Grounding, Soothing, Coping and Regulating Cards; Dr Karen Treisman, 2018 or Bear Feelings Cards; John Veekan, 2012), rich pictures and projective techniques.
- Consider the purpose of gaining the pupil’s views and the relevance of the resources being used and questions being asked to this purpose. Can, what a pupil has told you, be used to influence change and if not, how is this communicated to the pupils?
Pupil Voice and COVID 19
A range of completed and on-going studies exploring children and young people’s experiences during COVID 19 and lockdown has been identified by The Royal College of Paediatrics and Child Health. The voices of children and young people are central to recovery planning and the direction of future support and services.
Find downloadable resources with strategies to encourage pupil voice on the Devon County Council website:
Strategies to encourage pupil voice – Support for schools and settings (devon.gov.uk)
6.2. Working with parents and carers
Engaging parents and the wider community can take time and be resource intensive. Those who have had success in this area suggest the following strategies, but stress that they take time to develop. You may wish to consider how effectively these elements are embedded within your setting.
- Appoint a senior manager or learning mentor to be responsible for home-school liaison.
- Hold class meetings for new parents and drop-ins for all parents.
- Provide lifelong learning opportunities on the school premises, drawing on a wide network of service providers.
- The school should be aware of the diversity in the parent/carer group and adopt approaches which reach out to all parents. There may be a need for extra encouragement or support to enable them to be actively involved: family learning initiatives for example. It may be helpful to have staff members from the same ethnic backgrounds and who speak the same languages as local communities.
- Promote the school and its achievements among local community groups.
- Provide opportunities for pupils to volunteer in the community, for example visiting care homes for older people.
- Have an environmental or conservation club working in the community.
- Distribute the school magazine in the community.
There are a number of strategies which can be used to involve parents in whole school-work on emotional health and wellbeing.
- Ensure that the taught emotional health and wellbeing curriculum includes activities which pupils can complete at home with their parents.
- Share information about the school’s approach to emotional health and wellbeing in accessible and engaging ways on a regular basis.
- Hold workshops for parents to attend on topics pertinent to the age of their child such as separation anxiety, supporting friendships and healthy use of social media.
Parental involvement is also key when supporting children who are experiencing difficulties with their emotional health and wellbeing. It is essential that parents and carers are involved in any approaches used to support their child. Their views should be sought on initial planning and they should be kept informed throughout as the work develops. Their consent should be sought for any on-going support/referrals for outside agencies. The exception to needing parental consent is when the young person is not yet 16 but is in law, ‘Gillick competent’. Under particular circumstances, children aged under 16 can give consent for medical intervention without the involvement of their parents. The situation that this most often applies to in schools is the provision of counselling.
It is important to recognise that some parents and carers will themselves have emotional health and wellbeing needs which may affect their capacity to support child and / or impact on their own resilience.
7. Prioritise professional learning and development
In order to have a staff team who are effective in supporting the wellbeing of colleagues and pupils, they need to have learning and development opportunities to develop skills and knowledge in this area. Staff need training to understand the factors which impact on emotional health and wellbeing including:
- The impact of trauma and ACEs.
- Resilience including risk and protective factors
- Attachment
Have the staff in your setting received training in these areas? How can you prioritise this within your CPD plan?
This section contains information to support staff to understand the factors including emotional health and wellbeing and can be used as the basis of initial CPD.
7.1. Supporting staff to understand factors influencing EHWB
Resilience
All children are capable of working through challenges and coping with stress. However, wellbeing appears largely dependent upon our ability to be resilient in the face of adversity.
Resiliency can be defined as the ability to bounce back from stress, failure, challenges, or trauma. Resilient people continue to develop to their own potential even when circumstances are against them. It requires positive adaptation in circumstances where difficulties are so extreme that we would expect a person to be impaired (Masten, 2001).
Resiliency is regarded as being different from coping which is more closely linked to survival and is at a cost to one’s own healthy development.
There are two key factors that contribute to resilience. These factors are:
- Individual characteristics including gender, temperament, emotion regulation, cognitive skills, social skills, self-efficacy and self-esteem.
- Social / environmental including family, social support, school and community factors (Rutter, 1979).
Adverse Childhood Experiences (ACES)
Recently there has been much interest in the area of Adverse Childhood Experiences (ACES). Adverse Childhood Experiences (ACEs) are traumatic events that affect children while growing up, such as having a parent in prison, suffering child maltreatment or living in a household affected by domestic violence, substance misuse or mental illness (Felitti et al, 1998).
Research was initially published in the USA and later replicated in both England and Wales. The research found that there was a correlation between the number of adverse childhood experiences a person had and poor health and social outcomes in adulthood (Bellis et al, 2015).
It has long been recognised that stressful events occurring in childhood impact on children’s ability to learn and participate in school life. ACES can be regarded as being risk factors to a child’s physical and emotional wellbeing. ACES can cause feelings which can be overwhelming and distressing. The experiences and associated feelings can have a significant and negative impact upon the child’s presentation and performance in school.
Risk factors and protective factors
Not all children that experience adversity i.e. risk factors, will go on to develop difficulties with emotional health and wellbeing. Protective factors have also been identified which are associated with greater resilience and ultimately better lifetime outcomes. To explain this, it may be useful to imagine a pair of scales, which represent the wellbeing of the child, with one side of the scales representing risk factors and the other side representing protective factors.
It is important that the scales (child) remains balanced. This is achieved by having at least as many, preferably more, protective factors upon the scales (child) than there are risk factors. The greater the number and / or weight of the protective factors, the greater the child experiences resiliency and can maintain positive emotional health and wellbeing despite adversity.
Risk factors may include some of the following:
- Traumatic events that occur in childhood (0-17 years) such as experiencing violence, abuse or neglect.
- Aspects of the child’s environment that can undermine their sense of safety and stability, such as living in a household with instability, substance misuse or mental health difficulties.
- Loss, for example bereavement, parental split or loss of home.
- Illness / disability, for example foetal alcohol syndrome.
- Family context and parenting style.
- Economic deprivation and limited aspirations.
- Having an SEN or learning disability.
- Limited experience of social and emotional learning opportunities.
Protective factors that schools can provide include:
- Secure base – schools can provide a safe and happy experience through the physical environment and through the relationships they have with children.
- Education – providing a relevant, warm and inviting experience and enabling children to learn skills for employment and life in general.
- Friendships – developing positive relationships and a sense of belongingness, whilst helping to separate from unhelpful relationships.
- Positive values – illustrating these through the way staff interact with children, including how we incentivise and reward children.
- Social competencies – these can be taught and experiences offered to children to both learn and demonstrate these skills.
- Empowerment – supporting young people to have a voice i.e. via school councils.
- Physical activity and education around a healthy diet and lifestyle.
How can schools promote resilience in children and young people?
Research suggests that the following strategies can be used by school staff to promote resilience in pupils. The key factor in all of these strategies is the relationship between staff and pupils.
- Ensuring that the young person has access to least one trusted adult, over time. The adult is able to ‘hold the pupil in mind’ and let them know that they care.
- Preparedness and capacity to help with basics, i.e. food, clothing, transport, and even housing.
- Safe spaces – quiet, soothing spaces for pupils who wish to retreat from ‘busy’ school life.
- Making sure disadvantaged pupils actually access activities, hobbies and sports.
- Helping to map out a sense of future (hope and aspirations) and developing life skills.
- Helping to develop and practice problem-solving approaches at every opportunity.
- Help for pupils to process and manage their feelings.
- Creating a culture of Connection, Protection, Understanding and Care – in line with Relational Practice approaches (Dunnett and Jones, 2020)
- Support to help others e.g. volunteering, peer mentoring.
- Opportunities for all staff, pupils and parents to learn about resilience.
- A staff team who treat each other with care and respect, modelling the behaviour they expect from pupils.
Resources to promote resilience
We have developed guidance, training and support for schools wishing to implement Relational Approaches, Polices and Practice. Relational approaches focus on nurturing relationships between staff and pupils based on connection, protection, understanding and care which have been found to be key factors in building resilience and promoting emotional health and wellbeing. Please see Section 9 and 10 for further details.
There are many other practical resources available to Devon schools:
- The Educational Psychology Service have a range of assessments and training resources. An Educational Psychologist is able to undertake an assessment of a child’s / young person’s resiliency and offer a detailed profile. This will help to understand the child’s needs and will identify practical strategies to support resilience.
- Devon Educational Psychology Service provides training for Emotional Literacy Support Assistants (ELSA) and on-going supervision. Please contact one of the leadership team to find out about upcoming opportunities.
- Young Minds provide training and resources to develop academic and emotional resilience
7.2. Supporting staff to understand adolescent changes in the brain
It may be helpful for school staff, especially in secondary settings, to have an understanding of how the adolescent brain changes and how this may impact on wellbeing.
The brain reflects the world in which we have grown up. How we feel and respond to our feelings through behaviour is linked to underlying and unconscious physiological and emotional processes, which in turn are a product of our brain development.
The brain is a very complex organ comprised of many different regions including the cerebral cortex, limbic system, amygdala, hypothalamus and brain stem. There are complex interactions between the brain and the autonomic nervous system and hormones such as adrenaline, oxytocin and cortisol. (Dunnett and Jones, Attachment Based Mentoring (ABM) Programme, 2018).
Cerebral cortex
This is responsible for higher thought processes, for example, speech and language and perception, memory, attention, awareness, thought, reflection and consciousness.
Limbic system
This is sometimes referred to as the emotional centre of the brain because it is a collection of brain structures involved in a variety of functions including emotion, behaviour, motivation, memory and smell.
The amygdala
This is sometimes referred to as the alarm centre of the brain and is responsible for how we perceive and process emotions by storing and interpreting stimuli including fear inducing information from the environment.
The hypothalamus
This is part of the limbic system is responsible for linking the nervous system to the endocrine system (hormones) via the pituitary gland.
The brain stem
The brain stem is the posterior part of the brain continuous with the spinal cord. It has many basic functions including heart rate, breathing, sleeping and eating. The nerve connection of the motor (movement) and sensory systems from the main part of the brain pass through the brainstem to the rest of the body.
When we feel unsafe, physically or psychologically, impulses from the amygdala and brainstem can take over. Adolescents may at times behave like a frightened animal (fight / flight / freeze) and become anxious, impulsive or lash out with rage.
In order to support children and young people we must understand how to meet the underlying developmental needs and not just manage the symptoms (Dunnett & Jones, 2018).
The impact of adolescence
During adolescence there is a major increase in neurons in the frontal cortex – the part of the brain that has most to do with thinking, reasoning, logic and decision making. Far too many connections or synapses grow and they need to be cut back or pruned. This pruning is more important than the growth. Learning occurs when synaptic connections are strengthened and neurological pathways are formed. Pathways that are not used are lost.
For parents, teachers, and anyone who cares for a teenager – it is often difficult to help a teen navigate the broad range of challenges that accompany the complex changes occurring in the body, mind, and brain. This transition is riddled with many potential difficulties for many teenagers.
Teenage brain structure, connectivity, and behaviour are all intertwined. While young adults are advancing to new levels of sophisticated thinking and emotional regulation, their brains are simultaneously undergoing changes directly needed to support these functions.
So there is something about adolescence that makes it a unique period of development and behavioural change. We used to put the behaviours that we associate with the teenage years down to changes in the level of hormones, sex hormones at puberty, and also social changes, like going to a new school, from a small primary to a big secondary for example. But we now know that in addition to hormones and social effects, the brain is also undergoing a huge amount of change, and it’s the development of the brain that probably explains some of the typical teenage behaviours. (Blakemore 2018)
8. Implement targeted programmes and intervention
In addition to training staff in how to understand the factors influencing EHWB, schools need systems in place to ensure that difficulties with emotional health and wellbeing are identified early and interventions are put in place. The effectiveness of these interventions needs to be evaluated and where appropriate, changes made to either increase the amount or intensity of support provided or involve external professionals in thinking about what the child requires.
8.1. Understanding need, planning interventions and monitoring impact
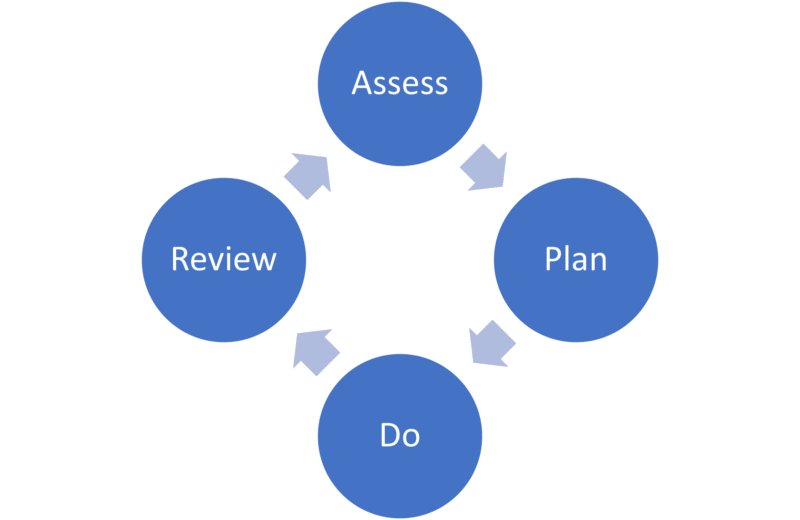
An ‘Assess, Plan, Do, Review’ cycle is part of the graduated approach for children and pupils with special educational needs and is equally applicable to supporting pupils with emotional health and wellbeing needs.
How well does your setting embed ‘Assess, Plan, Do, Review’ for children with emotional health and wellbeing need?
Assess
- Early identification of signs and symptoms of difficulties is crucial.
- Identify the pupil’s strengths and successes, in addition to their needs.
- Ensure you have gained pupil and parental perspectives.
- Assessment of emotional health and wellbeing should be sensitive and caring. Ensure you listen actively in a non-judgmental way.
- Use of visual resources such as scaling, strength or feelings cards, appropriate questionnaires etc. will be helpful.
- Recognise the importance of building a positive relationship with the pupil based on Relational Support Principles (Protection Connection, Understanding and Care).
- Consider the need for advice and assessment from external agencies if difficulties are severe.
Plan
- Agree the intervention required with the pupil, parents and key team around the child.
- Consider materials, differentiation, staffing and interventions needed for success
- Recognise the need for consistent positive support to build trust and create change and that this can take time.
- Keep a record using a provision plan / pastoral support plan / Relational Support Plan / emotional health and wellbeing plan or similar.
Do
- Consider who will be the best person to deliver interventions – consider the wishes of pupil.
- Focus on developing a positive relationship of mutual trust and respect.
- Put in place interventions, giving thought to how progress will be monitored.
- Encourage, praise and notice small gains.
- Consider in advance how any setbacks can be dealt with positively.
Review
- Review the effectiveness of intervention- note that long term changes can take time and consistent support and relationship building is key.
- Recognise strengths and successes as well as the difficulties that persist.
- If appropriate, increase the amount or intensity of support, or change and amend the support as appropriate.
- If difficulties persist, consider the need for advice and support from external agencies.
8.2. The Devon Graduated Response to SEND tool
The Devon Graduated Response to SEND support profile can be used as an electronic tool to support teachers and SENCOs to identify, assess and record the needs of children and young people requiring special educational provision. It supports the planning and recording of appropriate provision and provides guidance for reviewing progress. It has been designed to help educational settings meet their duties as outlined in the SEND Code of Practice.
It aims to ensure a graduated approach to meeting need through effective implementation of universal support before moving a child or young person onto higher levels of support by following the Assess, Plan, Do, Review cycles. How well is this tool used within your setting?
Devon’s graduated response – Support for schools and settings
8.3. Case study 1 – example of Assess, Plan, Do, Review
Kira is in Year 7 is at risk of Permanent Exclusion due to a series of serious incidents and persistent disruptive behaviour following her transition to secondary school. It is suspected that she is experiencing emotional health and wellbeing difficulties which are making it challenging for her to manage the demands of school.
Assess:
A Team Around the Family (TAF) meeting involving key members of school staff and Kira’s parents was held to gather information about risk and protective factors, and to plan intervention. An Interactive Factors Framework (IFF – see Appendix) was used to guide the discussion and record key points relating to Kira’s needs. In addition to this, Strengths and Difficulties Questionnaires (SDQ) were completed by Kira’s teachers and parents which consistently indicated a high level of risk regarding her emotional health and wellbeing.
Plan / do:
An intervention plan was agreed at the TAF based on the needs identified via the IFF and SDQ. This included a range of personalised strategies aimed at reducing the impact of risk factors and increasing access to protective factors. For example, opportunities were found for Kira to build relationships with adults, and to be given additional time to participate in activities where she is successful i.e. construction. Information was sent to all Kira’s teaching staff regarding best practice around supporting her with learning and behaviour. Kira was also offered weekly mentoring with a member of staff trained in Attachment Based Mentoring. It was agreed that all parties involved in delivering support would feedback briefly by email on a weekly basis, to help monitor whether the interventions were working for Kira and whether any changes needed to be made.
Review:
It was agreed at the first TAF that Kira’s progress would be reviewed in 6 weeks. In order to review progress, the school’s SENCo collated exclusion data, repeated the SDQ and gathered Kira’s views alongside the views of staff who were unable to attend the review. No exclusions were recorded during the six-week period and there was a reduction in minor incidents. Information from school staff including SDQ data indicated positive progress, however parents reported struggling with Kira at home, and their parental SDQ ratings were still high. This provided a focus for the next cycle of assess-plan-do-review, with family intervention being introduced alongside ongoing school-based support.
8.4. Tools to support identification, assessment and interventions for emotional health and wellbeing difficulties in schools
Assessment tools
The following tools can be used by staff in your setting to identify and understand the emotional health and wellbeing needs of pupils:
- Spence Anxiety Scale – A questionnaire to identify levels / areas of anxiety for children aged between 8 and 15 years. There are separate questionnaires for the child, parents and teachers to complete so that information from different sources can be compared. This can be completed and scored by school staff but should be interpreted by a professional with additional training in wellbeing and mental health. https://www.scaswebsite.com
- Strengths and Difficulties questionnaire – This questionnaire can identify strengths and difficulties linked to wellbeing for children aged between 3 and 16 years. It can be completed by parents and school staff and scored online, however, the results should be interpreted by a professional with additional training in wellbeing and mental health. https://www.sdqinfo.org/a0.html
- Boxall Profile – This two-part checklist identifies the SEMH needs of children and young people and highlights the skills they may possess or lack in order to engage with learning. The Boxall Profile supports the ‘assess, plan, do, review’ processes; helping with early identification and assessment, target setting and provision development, tracking and reviewing progress. https://new.boxallprofile.org
- The Inclusion Toolkit – No Need to Exclude: Working together to end exclusions in Devon – Page 29 of this guidance contains further evidence-based assessments to identify children and young people with emotional health and wellbeing needs. Inclusion toolkit (No need to exclude) – Support for schools and settings (devon.gov.uk)
- Interactive Factors Frameworks (IFF) – This tool supports teachers to analyse and unpick the needs of children and young people who they have concerns about. It prompts staff to consider how biological, cognitive, behavioural and environmental factors may interact and supports staff to understand why a young person may present with certain behaviours. See the Appendix for blank template of the IFF plus an example.
- Relational support plan – The Relational Support Plan provides a framework for exploring the needs of vulnerable children and young people, including those in care. It draws upon evidence showing that feeling secure and having positive relationships are essential to wellbeing, behaviour and learning. Relational learning – Support for schools and settings (devon.gov.uk)
- Speech, Language and Communication needs: Data indicates that many children and young people with SEMH needs have unidentified Speech, Language and Communication needs. Schools can use their own screening processes and consider a referral to a Speech and Language Therapist.
Interventions
You may want to consider whether your setting is using evidence-based interventions and how you measure the impact and effectiveness of the interventions you are using.
Evidence-based programmes for a range of needs and ages:
- The Early Intervention Foundation Guidebook provides information about early intervention programmes that have been evaluated and shown to improve outcomes for children and young people. Schools can search for evidence-based programmes to support the EHWB of students. https://guidebook.eif.org.uk/search
- The Education Endowment Fund also provides evidence-based interventions for developing social and emotional skills at universal, targeted and specialist levels. https://educationendowmentfoundation.org.uk/evidence-summaries/teaching-learning-toolkit/social-and-emotional-learning/
- The Educational Psychology Service conducted a review of the literature and research into interventions for children with social, emotional and mental health needs and has produced the following document which outlines evidence-based interventions within a graduated response. The SEMH Toolkit.
Whole school / universal interventions
- The Social Emotional and Mental Health Advisory team can offer support, advice and training around a range of stress management techniques including the Massage in Schools Programme (MISP), Emotional Freedom Technique (EFT Tapping), mindfulness and meditation Contact us to find out more: Social, emotional and mental health (SEMH) – Support for schools and settings (devon.gov.uk)
- Emotional logic – Emotional Logic is a structured way to understand the useful purposes of emotions and the ability to turn unpleasant emotions into positive action whilst limiting distress and confusion. This life-long learning method leads to emotional strength and resilience in the face of life’s challenges. The Emotional Logic Centre is working in partnership with us to deliver Emotional Logic training and support to schools in Devon. Emotional Logic – Support for schools and settings (devon.gov.uk)
- Mental health first aid training for individual staff or whole organisations can support staff to have:
- An in-depth understanding of mental health and the factors that can affect wellbeing.
- Practical skills to spot the triggers and signs of mental health issues.
- Confidence to step in, reassure and support a person in distress.
- Enhanced interpersonal skills such as non-judgemental listening.
- Knowledge to help someone recover their health by guiding them to further support – whether that’s self-help resources, through their employer, the NHS, or a mix.
- Staff supervision – Research indicates that supervision for school staff can support their wellbeing and development by providing emotional support and facilitating problem solving when faced with sensitive and complex issues. This can be provided by both the Devon Educational Psychology Service and SEMH Advisory team.
Targeted and specialist intervention
- Free2BMe – A two day training course designed to equip school staff to deliver a structured 8-week intervention programme to groups of children who have been affected by domestic violence and abuse. The programme aims to support the development of emotional expression, sense of belonging, resilience, as well as practical tools such as learning how to keep safe. The hour-long sessions are aimed at children in Key Stage 2 and are designed for groups of between 6–8 children. Factors such as confidentiality, consent and communicating with families are discussed. This explores the cycles of dysfunctional relationships and how to promote healthy relationships. It has been developed, piloted and rigorously evaluated by the SEMH Team and Educational Psychology Service.
- Attachment Based Mentoring – ABM is a relational approach to supporting children with their social and emotional development. The approach includes both universal and targeted support, particularly for children who may have had adverse childhood experiences, those who are struggling with their emotional health and wellbeing and those who are finding it difficult to engage with learning and the social aspects of school. Attachment Based Mentoring training is available from Devon Education Services.
Interventions for parents
There are numerous interventions offering support for parents whose children may be experiencing EHWB challenges including:
The Overcoming Anxiety Programme for parents
- This is a guided Cognitive-Behavioural Therapy (CBT) programme for parents of anxious children which supports parents to become anxiety management experts who can continue to use the strategies they have learned to help their child after the intervention has finished.
- The Educational Psychology Service can run this programme for individual parents or small groups of 6-8 parents.
Services, support and consultancy – Support for schools and settings (devon.gov.uk)
Parenting courses
There are a range of parenting course available throughout Devon run by different organisations. They are usually free and can be found on the Pinpoint Devon website – https://www.pinpointdevon.co.uk/
Courses include:
- Solihull parenting
- Patchwork parenting
- The Strengthen Families Programme
- Parent Plus Adolescents Programme
9. Develop supportive policy
In order to truly promote positive emotional health and wellbeing, schools need inclusive and nurturing polices based around relational practice.
A growing number of Local Authorities and Schools are replacing traditional Behaviourist behaviour management approaches and polices with Zero-Exclusion polices and Relational approaches to teaching and learning. For example, Hope School in Liverpool, a special school for pupils with Social, Emotional and Mental Health Difficulties (SEMH) has a non-exclusion policy and has replaced the school’s Behaviour Management policy with a Relational Support for Personal Development policy. Hope School now focuses on attachment friendly practice and is focused on developing pupils’ intrinsic motivation.
The school’s OFSTED report (2019) states:
Based on academic research you have developed a school that is sensitive to supporting pupils with attachment and complex trauma histories. This new approach removed reliance on external sanctions and rewards to control behaviour. The emphasis changed to understanding the internal reasons for behaviour. … The impact of this new approach has been the creation of a school focused on understanding why pupils struggle to control their behaviour.…Behaviour in school is exemplary and pupils make outstanding progress in their learning.
The new OFSTED inspection framework places high importance on staff and pupil wellbeing, of which relationships are a key factor. It is hoped that many schools will follow suit and apply Relational approaches, policy and practice.
9.1. Roles and responsibilities
All members of school staff should understand their general responsibilities for ensuring the emotional health and wellbeing of their pupils. These will be established through safeguarding procedures, school policies and practices, the taught curriculum and specific emotional health and wellbeing initiatives (DfE, 2018).
School leaders and governors
School leaders and governors are responsible for ensuring that there is a clear vision for emotional health and wellbeing and that all aspects of school life effectively contribute to achieving this vision. This could include the following:
- The governing body and school leadership set a culture that values and includes all pupils enabling them to talk about problems in a non-stigmatising way.
- Emotional health and wellbeing is referenced in school improvement plans and policies. Plans and policies are monitored and evaluated.
- Leaders promote equality of opportunity and diversity for pupils and staff, so that the ethos and culture of the whole school / setting prevents any form of direct or indirect discriminatory behaviour.
- Leaders, staff and pupils do not tolerate prejudiced behaviour and challenge any examples of such.
- Leaders and staff have created a culture of vigilance where pupils’ welfare is actively promoted. Pupils are listened to and feel safe.
Strategic lead for emotional health and wellbeing
Strategic leadership of emotional health and wellbeing is essential to effective practice, and in coming years will be subsumed within the role of the Designated Mental Health Lead described in the Green paper ‘Transforming children and young people’s mental health provision’ (DoH & DfE, 2017).
The proposals suggest that the designated lead for mental health:
- Oversees the support the school gives to pupils with mental health problems.
- Helps staff to spot pupils who show signs of mental health problems.
- Offers advice to staff about mental health.
- Refers children to specialist services when needed.
Prior to these changes, schools are encouraged to consider their arrangements and to ensure that these are effective. Schools may choose to include these responsibilities within the role of a Special Needs Coordinator, Inclusion Coordinator or Pastoral Lead. The Strategic Lead for Emotional Health and Wellbeing should be part of the senior leadership of the school.
Form tutor / class teacher
The role of the form tutor in secondary education and class teacher in primary education is central to ensuring the emotional health and wellbeing of pupils. The form tutor/ class teacher is often the member of staff who sees a child or young person most regularly and may be the only staff member to spend ‘non curriculum’ time with the pupil. The role includes caring for students and, crucially, monitoring their progress both academically and socially, along with encouraging involvement, commitment and high standards of work and behaviour. The form tutor / class teacher should be active in looking after the interests of the ‘whole child’ and should understand and be aware of how to identify areas of concern with regard to their development and the school policy for responding to these concerns.
How effectively do staff understand and undertake their roles and responsibilities linked to emotional health and wellbeing in your setting?
10. Link emotional health and wellbeing to behaviour management approaches
Behaviour management approaches are traditionally based around Behaviourist principle of rewards and sanctions and can be punitive and re-traumatising for children who have experienced adverse childhood experiences. Relational approaches are based on attachment principles and regulatory and restorative approaches which are more effective in supporting the development of internal control and regulation.
What approach to behaviour management is used in your setting?
10.1. Relational approaches to teaching and learning
Secure relationships have a direct bearing on children’s capacity to succeed in school. Relationships and belonging are key to success for all children and essential for those who have experienced relational losses and trauma. A child’s behaviour should always be understood in the context of underlying needs and adverse experiences which may be impacting on the emotional health and wellbeing. Children and young people often communicate their distress via their behaviour whether this is ‘acting out’ or more withdrawn types of behaviour.
Schools can be huge protective factors for children and young people who have experienced ACES and trauma; supportive and positive relationship with school staff are key to this. Understanding relational learning provides a framework for whole school development and universal provision, as well as for those who have the greatest need.
Devon Education Services offer a range of support and training packages to develop Relational Approaches, Policy and Practice in schools including support for senior leadership to develop Relational policies and practice, whole school training and the development of assess, plan, do review processes using a Relational Support Plan.
These approaches have a following core aims:
- To develop an understanding of how adverse experiences and trauma may impact on emotional development and wellbeing.
- To raise empathy and understanding for children who may be finding school hard.
- To develop whole school practice, procedures and policy aligned to relational learning.
- To enable the adults working with children to be able to read their behaviour in terms of underlying needs and provide for these needs in terms of what they are doing and how they are being with them.
- To support adults to develop the skills they need to form secure relationships with the children they work with, use coaching skills to support their development and practical skills to support their inclusion.
- To support adults to become reflective practitioners who can be responsive to children’s needs and adapt to different situations.
The Virtual School for Children in Care have commissioned the development of Guidance for Developing Relational Practice and Policy which is accessible to all schools on the Devon County Council website. Relational learning – Support for schools and settings (devon.gov.uk)
- Guidance for Developing Relational Practice and Policy aims to support the inclusion, engagement and outcomes for all children and young people with a particular focus on those who are vulnerable to and at risk of exclusion. The guidance was written in response to well documented concerns regarding young people’s mental health and well-being and long-standing national trends which show the disproportionate exclusion of children from vulnerable groups.
- The document describes an approach to teaching and learning which influences whole school ethos and systems as well as universal teaching practice and targeted support. It supports the development of Relational Behaviour Policies which take into account current research and theory from the fields of attachment and trauma, effective support for inclusion and on improving behaviour in schools.
- There are three main components to the relational model, Developing Relationships, Responding and Calming and Repairing and Restoring as well as guidance on working in relationship in the classroom and through a graduated response. The approaches should be used universally as good quality first teaching and in a planned and timely fashion to target early intervention for children and young people who may be at risk of exclusion.
11. Implement targeted responses and identify specialist pathways
When supporting the EHWB of children and young people it is important that a graduated response is taken. This involves accurate and early identification of support and the appropriate level of support being implemented and reviewed. For most children and young people ‘universal’ support will be sufficient; however, some children and young people whose needs may be more complex or intense will require targeted or specialist support.
The Emotional Health and Wellbeing Pathway has been developed in partnership with colleagues from CAMHS, School Nursing and Public Health to support education settings to identify need, implement effective interventions and source appropriate external support in a graduated way. The Pathway follows the I THRIVE Framework which is a person centred and needs led approach to supporting mental health needs.
11.1. The emotional health and wellbeing pathway
Level of need – THRIVING – universal level
Most children and young people thrive and cope with the ‘normal’ difficulties and challenges of life and of growing up. They usually cope with challenges using their own resilience, the support of family and friends and support from their school.
Children and Family Health Devon – https://childrenandfamilyhealthdevon.nhs.uk/
Pinpoint Devon: https://www.pinpointdevon.co.uk/
Devon County Council: https://www.devon.gov.uk/education-and-families/send-local-offer/
What can the school / setting do?
- Develop and publish a Mental Health Strategy which focuses on resilience and wellbeing of both staff and students.
- Involve parents and pupils in decision making and policy development.
- Promote an emotionally healthy whole school environment which includes Mental Health Ambassadors, peer mentors etc.
- Use PSHE delivery (Rise Above for Schools) to raise awareness and promote emotional health and wellbeing.
- Embed 10 a day for Mental Health.
- Have effective and supportive policies on Inclusion, anti-bullying.
- Employ Relational Approaches to teaching and learning and develop a Relational Behaviour Policy. Relational learning – Support for schools and settings (devon.gov.uk).
- Have a system of early identification and support i.e. re early absence, changes in behaviour / engagement in learning, early transition planning and support.
- Individual Health Care plans and reasonable adjustments for known health conditions/ SEND (and staff training on identification and management of these needs).
- Anna Freud Schools in Mind Network https://www.annafreud.org/schools-and-colleges
- Staff training – MH First Aid, EH4MH, MindEd https://www.minded.org.uk/
- https://www.mentallyhealthyschools.org.uk/
- Useful Resources include: We Eat Elephants, My Big Life and Living Life to the Full https://www.fiveareas.com/
- Solihull Parenting Online https://www.inourplace.co.uk (access code TAMAR)
Community and national support
Community support
- Early Help: https://www.devonscp.org.uk/early-help
- Children’s Centre for 0-8
- ChatHealth (text a Devon SN 11-19yr olds) 07520631722
- Space Youth Centres: https://www.spaceyouthservices.org/
- Devon Young Carers: https://devoncarers.org.uk/am-i-a-carer/young-carers-2/what-happens-at-devon-young-carers/
- Prevent: https://saferdevon.co.uk/
National support
- Place2Be: https://www.place2be.org.uk/
- Young Minds: https://youngminds.org.uk/
- Rise above (for young people): https://riseabove.org.uk
- The Mix (for under 25s) call 0808 808 4994 https://www.themix.org.uk
- YSmart: http://ysmart.org.uk/
- LGBTQI: https://www.intercomtrust.org.uk, https://www.youngstonewall.org.uk/lgbtq-info
- Show Racism the Red Card: https://www.theredcard.org/
Level of need – GETTING ADVICE: targeted support
Some children and young people (CYP) show signs of emerging mental health needs and / or are struggling with their emotional well-being. Problems may be outside the normal range for their age or gender and of a mild to moderate nature. These will be starting to cause difficulties with their schoolwork, friendships or family relationships.
Happy Maps: Reliable Resources to support Emotional Health and Wellbeing – https://www.happymaps.co.uk/
What can the school / setting do?
In addition to the previous support….
- Explore concerns with parents and the CYP
- Be alert to signs of emerging emotional problems; use data and evidence-based tools to assess such as the Devon Graduated Response document, Emotional Health and Wellbeing Offer, and No Need to Exclude Guidance, to identify pupils who need targeted school-based or community interventions.
- Inclusion toolkit (No need to exclude) – Support for schools and settings (devon.gov.uk)
- Consider whether there are other needs that require support i.e. is it an emotional response as a normal reaction to a stressful situation or unmet need (individual, family or environmental)?
- Refer to the School Nurse: https://www.devon.gov.uk/educationandfamilies/health/public-health-nursing
- Consider referring to School Counsellor, Educational Psychologist, SEMH Advisory teacher.
Community and national support
Community support
- Integrated Children’s Services – CFHD.DevonSPA@nhs.net or phone on 03300 245 321.
- Counselling – Self-referral for online emotional wellbeing support and counselling – https://www.Kooth.com
- Young Devon – https://www.youngdevon.org/what-we-do/mental-health-well-being
National support
- Child line: 0800 1111 https://www.childline.org.uk
Level of need – GETTING HELP: specialist support
A few CYP will show signs of significant mental health problems that impact on daily activities and prevent them from functioning within the norms for their age.
These may be persistent and moderate to severe in nature, causing significant difficulties with their achievement and relationships.
What can the school / setting do?
In addition to the previous support…
- Continue to use school-based interventions to support the pupil.
- Contact CAMHS pre-referral helpline for advice / consultation and follow advice given (this may be to refer in for CAMHS specialist support).
- Consider consultation with an Educational Psychologist – https://www.devon.gov.uk/support-schools-settings/send/educational-psychology/
- Consider any Safeguarding concerns / implications – Safeguarding in schools – Devon Safeguarding Children Partnership (devonscp.org.uk)
Community support
- Specialist CAMHS – Single Point of Access (CAMHS- SPA): TSDFT.DevonSPA@nhs.net on 0330 0245 321
- Devon Safeguarding Children Partnership – https://www.devonscp.org.uk/health-and-wellbeing/emotional-and-mental-health
National support
- NHS – 111
- Shout – Text ‘SHOUT’ to ‘85258’ for crisis support via text.
Level of need – GETTING MORE HELP: urgent mental health support
This may be needed for serious mental health crisis (e.g. psychosis), suicidal ideation or serious weight loss and signs of an eating disorder.
CYP with complex and significant learning needs may express their mental health needs via challenging behaviour or detachment / withdrawal. Seek support from the Learning Disability team. You may need to contact the Police if behaviours are aggressive.
Follow safeguarding procedures.
What can the school / setting do?
In addition to the previous support…
- Contact parents immediately unless you have safeguarding concerns that would increase the risk to the child/young person by discussing with the parent/carer.
- Contact CAMHS-SPA on 0330 0245 321 for advice and for a decision on the urgency of the mental health need.
- After 5pm, contact 0300 555 5000 or the out-of-hours GP service by dialling NHS 111
- Or take to Accident and Emergency
Community and national support
Community support
- If a child is in immediate danger contact the Police on 999.
- If a child or young person is in need of protection or safeguarding contact Devon Multi-Agency Safeguarding Hub (MASH). Ring 0345 155 1071 or email mashsecure@devon.gov.uk
- Consider Exploitation – https://www.preventingexploitationtoolkit.org.uk/
National support
NSPCC – https://www.nspcc.org.uk/keeping-children-safe/our-services/nspcc-helpline/ 0808 800 5000
Level of need – getting risk support
Emergency medical help needed to preserve life following life-threatening self-harm
- Call the Police if CYP has absconded or is expressing suicidal ideation.
- DSCP provide further guidance on suicide prevention https://www.devonscp.org.uk/health-and-wellbeing/suicide-awareness/
What should the school / setting do?
In addition to the previous support…
- Contact parents immediately unless you have safeguarding concerns that would increase the risk to the child/young person by discussing with the parent/ carer.
- Call 999
- CAMHS assessment would be undertaken in A&E
- Check in with CYP and parent following an incident and identify support in school should they want this.
- Refer to Self-Harm Guidance for Schools on Devon County Council Support for Schools and Settings website.
Community support
- Pete’s Dragons provide post suicide support for families and schools – http://www.petesdragons.org.uk/
- CAMHS – 0330 0245 321
- Devon Educational Psychology Service – school support for suicide/bereavement
- Critical incident pack for schools – Support for schools and settings (devon.gov.uk)
National support
- Winston’s Wish –Bereavement support – https://www.winstonswish.org/
- Papyrus – Suicide Prevention for schools – https://papyrus-uk.org/wp-content/uploads/2018/08/toolkitfinal.pdf
11.2. Case study two – an example of a Graduated Response to EHWB
Chloe is in Year 3 and her class teacher has become increasingly concerned about her emotional wellbeing. Chloe is withdrawn, appears to have few friends and there are concerns about high levels of stress within the family due to poverty and social isolation.
After an initial assessment of her needs and consultation with Chloe and her parents, the following interventions were put in place.
Universal provision:
Chloe will be part of a small group of children that receive support from a Higher Level Teaching Assistant (HLTA) who has received training in supporting emotionally vulnerable children. The group meet once per week at break time and once per week in the afternoon. The group focuses on friendships and feelings. Chloe has been allocated a place at Lunch Club. A referral to Early Help was made with a request for funding so that Chloe can attend Breakfast Club, which was agreed. All staff within the school were made aware of Chloe’s needs.
Targeted support:
Further assessment of Chloe’s emotional needs was undertaken by the school SENDCo using a range of evidence-based tools including the Boxall Profile. The outcome of this assessment indicated several areas of vulnerability and as such, it was felt that Chloe would benefit from a more intensive period of intervention. In addition to the universal provision available Chloe received weekly 1:1 sessions with the HLTA for an initial period of 8 weeks. The HLTA also established regular communication with the family, leading to securing a Family Support Worker to work with the family via Early help.
Specialist support:
When the interventions were reviewed, Chloe made some small observable steps of progress however her class teacher and HLTA were still extremely concerned about her wellbeing. She appeared highly anxious, disengaged with learning and there were concerns about self-harming behaviours. A second assessment using the Boxall Profile did not indicate significant shifts and it was therefore felt Chloe needed specialist assessment and intervention. A referral to the Educational Psychology Service and CAMHS was made. The Educational Psychologist was able to provide further advice and support to staff on how they could best meet Chloe’s needs within the school environment. Chloe is awaiting her initial appointment with the CAMHS team.
12. Emotional health and wellbeing support from local agencies and organisations
After implementing an Assess, Plan, Do, Review cycle and following a graduated response, support from external professionals should be sought in the following circumstances:
- School based interventions have not resulted in sufficient progress in the difficulties experienced by the pupil.
- The difficulties experienced by the pupil are beyond the expertise or experience of the school.
- The difficulties experienced by the pupil are such that they are at risk of harm to themselves or others.
In the event of safeguarding concerns schools should call the Multi Agency Safeguarding Hub (MASH)) on 0345 155 1071 or email mashsecure@devon.gov.uk.
There are a range of external agencies in Devon who schools can seek support from if they have concerns about a child or young person’s emotional health and wellbeing.
Child and Adolescent Mental Health Service
Devon CAMHS provide specialist and evidence-based interventions to all children and young people in Devon, under the age of 18, who are experiencing severe, complex and enduring mental health and emotional wellbeing problems. https://childrenandfamilyhealthdevon.nhs.uk/camhs/professional/
Where symptoms are displayed mainly through behaviour, the referral should include information on what strategies and interventions have already been put in place and the impact of these in order to ascertain whether the need is felt to be related to the mental health of the child, rather than other factors in their life and environment.
Prior to a referral to CAMHS schools can call the pre-referral phone line at the Single Point of Access (SPA) to speak to a CAMHS Clinician regarding their concerns and they will advise on next steps and whether a CAMHS referral is appropriate. Contact the SPA on 0330 0245 321.
Referrals can be made online by completing the Request for Service form. http://childrenandfamilyhealthdevon.nhs.uk/camhs/professional/professional-support/request-criteria-camhs/
Early help
Early Help is an approach which brings together a range of service and professionals to support children, young people and families. https://www.devonscp.org.uk/early-help/
School nursing
The School Nursing Service provides information and support to school-aged children and their families who live in Devon or who attend a Devon school. Schools can contact their locality team for support and advice: https://www.devon.gov.uk/educationandfamilies/health/public-health-nursing-school-nursing
South – 0333 234 1901 southerenphnhub@nhs.net
Exeter – 0333 234 1902 exterphnhub@nhs.net
East – 0333 234 1903
North – 0333 234 1904
Devon County Council
Have a range of school support services including:
Educational Psychology Service – The EP service is a team of trained educational psychologists working across the county who can support schools and settings in a wide range of areas including individual assessment and intervention, whole school training, staff supervision and coaching, strategic work with senior leadership and project work/research focusing on EHWB.
Social Emotional and Mental Health Advisory Team – The SEMH team (previously known as the Behaviour Support Team) provides an early help service to schools. They work on a case-by-case basis supporting school staff to develop provision and practice which meets the SEMH needs of children who are finding school difficult and who may be at risk of exclusion. The team can help schools to understand children’s needs and provides advice, guidance, resources and training designed to meet those needs. Their key service aim is to support the inclusion of vulnerable and at- risk students, reducing risk and improving both their well-being and their educational progress and attainment. The team are able to support the development of staff groups with a range of tried and tested bespoke training options.
Schools and settings are encouraged to make a request referral to the SEMH team when a child’s emotional health and wellbeing is having a negative impact on their ability to meet behavioural expectations, access the curriculum and make appropriate academic progress and where their behaviour is a health and safety concern and puts the child at risk of exclusion. The SEMH team encourage early intervention which aims to meet children’s needs without need for an EHCP, however they are able to provide statutory advice when they have been involved in the plan, do, review cycle over time and a statutory plan is essential to meet a child’s needs in a mainstream setting.
Communication and Interaction Team (C&I) – The C&I Team is a Specialist Support Service consisting of highly qualified and experienced Specialist Teachers, a Pre-5 Specialist and Specialist Support Assistants who support the work with children and young people who have autism and / or speech, language and communication needs (SLCN). The C&I teamwork in partnership with schools and other settings to promote presence, participation and achievement and to secure better outcomes for children and young people with C&I needs across Devon. This is done through helping staff in schools and settings to understand the learning, emotional wellbeing and behaviour of children and young people to develop strategies to support them more effectively, enabling them to reach their potential.
Private practitioners
Support is also available from private practitioners. Schools need to ensure that private practitioners have suitable qualifications and experience for the work being undertaken and are registered with appropriate regulatory bodies such as the Health and Care Professionals Council or the British Association for Counselling and Psychotherapy.
Kooth
The Kooth.com website is accessible to children and young people in Devon aged 11-19. The site is staffed by fully trained and qualified counsellors and is available until 10pm each night, 365 days per year. It is free, safe, and confidential. It provides a non-stigmatising way for young people to receive counselling, advice and support on-line. https://www.kooth.com/
Space Youth Centres
Space provide 8 Youth Centres across Devon which are open evenings and weekends to support children and young people and provide them with a ‘safe space’ and a range of opportunities. https://www.spaceyouthservices.org/
Young Devon
Young Devon is a charity that supports young people across Devon with a range of services including accommodation and skills development. Relationships are at the heart of everything they do; they support young people to have a voice, promote wellbeing and can provide counselling for young people experiencing mental health difficulties. https://www.youngdevon.org/
YSmart
Drug and Alcohol Support for under 18s. https://ysmart.org.uk/
Bereavement charities
- Balloons is a charity supporting pre and post bereaved children, young people and families in Devon. https://www.balloonscharity.co.uk/
- Pete’s Dragons is a charity providing comfort for children and families after suicide loss. Pete’s Dragons also provide support and guidance for schools and settings. http://www.petesdragons.org.uk/
13. Emotional health and wellbeing support from national agencies and organisations
Anti-bullying
Bereavement:
LGBTQI
Mental health:
- https://www.youngminds.org.uk
- https://www.childline.org.uk/
- https://www.nspcc.org.uk
- https://www.ncb.org.uk/
Recognition of School Emotional Health and Wellbeing work
School counselling
Self-harm
- https://www.selfharm.co.uk – there is further guidance for schools regarding self-harm on the Devon County Council website including: a Risk Assessment Tool, How to Create a Safety Plan and a Flow Chart documenting steps that should be taken by the school following an incident of self-harm.
Suicide in young people
Trauma recovery
Whole school approaches to Emotional Health and Wellbeing:
- https://www.thriveapproach.com/
- https://www.emotioncoachinguk.com/
- https://www.mindfulnessinschools.org/
- https://www.emotionallogiccentre.org.uk/
14. Jargon buster / glossary
Adverse Childhood Experiences (ACES): Are potentially traumatic events that occur in childhood including experiencing violence, abuse or neglect. ACEs include aspects of the child’s environment that can undermine their sense of safety and stability, such as living in a household with instability, substance misuse or mental health difficulties.
Attention Difficulties / Hyperactivity: Includes finding it hard to concentrate or stay still, being easily distracted.
Advocate: An individual who supports and speaks out on behalf of a parent, child or young person.
Alternative Provision (AP): Offers a different educational option for some pupils to access a broad curriculum which meets a range of different needs and interests.
Annual Review: A meeting that takes place at least once a year to look at the details of a child’s Education, Health and Care Plan, to record their progress and plan for the next year ahead and the future.
Child in Care (CiC): A child who has been in the care of their Local Authority for more than 24 hours. A chid in care is subject to some form of legal order and is placed with foster carers, in a residential home or with parents or other relatives (under certain circumstances).
Child in Need (CiN): According to the 1989 Children Act, a Child in Need either a) is unlikely to achieve/maintain a reasonable standard of health and development without Local Authority provision; or b) is likely to be impaired without local authority provision; or c) is disabled.
Children and Adolescent Mental Health Services (CAMHS): Devon CAMHS provide specialist interventions and evidence-based interventions to all children and young people in Devon, under the age of 18, who are experiencing severe, complex and enduring mental health and emotional wellbeing problems
Early Help: Early Help is not a specific service or team; it is an approach that brings together people from a range of services and teams who will work together to help to improve the situations for families in need of extra support.
Education, Health and Care Plan (EHCP): A statutory document drawn up by the Local Authority, setting out the education, health and social care support to be provided to a child or young person with Special Educational Need or a disability.
Educational Psychologist (EP): A psychologist who works with children, schools and families to remove barriers to learning and wellbeing.
Elective Home Education (EHE): A term used to describe a choice by parents to provide education for their children at home, or in some other way of choice, instead of sending them to school full-time.
Emotional Health and Wellbeing (EHWB): Describes how we think, feel and relate to ourselves and others and how we interpret the world around us. Good emotional health and wellbeing is about being positively engaged with the world and having strong sense of self-esteem.
Emotional Literacy: The ability to understand and express feelings. This involves having self-awareness, recognising one’s own feelings and knowing how to manage them.
Fixed Term Exclusion (FTE): When a child is excluded from an education setting for a specific period of time.
Free School Meals (FSM): In England, a Free School Meal (FSM) is a statutory benefit available to school-aged children from families who are on a low income. It enables children to have a meal provided by the school, free of charge.
Internal Exclusion: When a child is sent away from their usual classes within the school for a fixed period of time.
Local Offer: The Local Offer provides information on what services children, young people and their families with special education needs and disabilities can expect from a range of local agencies, including education, health and social care.
Mental Health: A state of wellbeing in which every individual reaches his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully.
Mental Health Champion or Lead: An identified and trained designated senior lead within schools to oversee the approach to mental health and wellbeing.
Mental Health Support Teams (MHSTs): Introduced in December 2017, MHSTs work with children and staff in education settings to provide extra capacity to deliver evidence-based psychological interventions in schools and create better links with wider services.
Not in education, employment or training (NEET): Refers to a young person who is unemployed, not in school or vocational training between the ages of 16 and 24 years.
Off Rolling: The practice of removing a child from the school roll without a permanent exclusion which includes pressuring parents to move their child to another school and / or to home educate.
Outcome: The benefit or difference made as a result of an intervention or service provided.
Permanent Exclusion (PEX): When a child is permanently excluded from a school or setting and is unable to return.
Preparing for Adulthood (PfA): Work to ensure that young people with SEND achieve paid employment, independent living, housing options, good health, friendships, relationships and community inclusion.
Protective Factors: Characteristics or attributes in individuals, families or communities that lessen or eliminate risk, thereby increasing the health and wellbeing of children and families.
Pupil Referral Unit (PRU): Local Authority funded school specifically for pupils who otherwise would not receive a suitable education. It is a short-term provision, usually accessed by pupils who have been permanently excluded.
Risk Factors: Characteristics or attributes in individuals, families or communities that precede and are associated with risk and a higher likelihood of negative outcomes.
Social, emotional and mental health (SEMH): Includes social and emotional functioning, wellbeing, the ability to regulate self and behaviour and mental health difficulties. This term has superseded Emotional and Behavioural Difficulties (EBD) since the publication of the 2015 SEND Code of Practice.
Special Educational Needs and Disabilities (SEND): A child or young person has special educational needs if they have a learning difficulty of disability which calls for special educational provision to be made for them.
Special School: A school that supports children with complex Special Educational Needs when education in a mainstream school is unable to meet their needs. All children attending have an EHCP.
Youth Justice Service (YJS): A team that supports children and young people who have committed offences and have come to the attention of the police.
15. References
Bellis, M. A., Ashton, K., Hughes, K., Ford, K., Bishop, J., and Paranjothy, S. (2015) Adverse Childhood Experiences and their impact on health-harming behaviours in the Welsh adult population. Cardiff: Public Health Wales.
Blakemore, S. J. (2018). Avoiding social skills in adolescence. Current directions in Psychological Science. 27 (2) 116 -122.
Bowlby, J. (1969). Attachment and Loss, Vol. 1: Attachment. Attachment and Loss. New York: Basic Books.
Children’s Society. (2017). The Good Childhood Report 2017.The Good Childhood Report | The Children’s Society (childrenssociety.org.uk)
Department for Education (2017). Supporting Mental Health in Schools and Colleges. DfE. https://www.gov.uk/government/publications/supporting-mental-health-in-schools-and-colleges
Department for Education. (2018). Mental health and Behaviour in Schools. DfE
Department for Education. (2018a). Permanent and fixed-period exclusions in England. https://www.gov.uk/government/statistics/permanent-and-fixed-period-exclusions-in-england-2016-to-2017
Department for Education. (2019). Relationships education, relationships and sex education (RSE) and health education: Guidance for governing bodies, proprietors, head teachers, principals, senior leadership teams, teachers. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/805781/Relationships_Education__Relationships_and_Sex_Education__RSE__and_Health_Education.pdf
Department of Health & Department for Education. (2017). Transforming children and young people’s mental health provision: A green paper. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/664855/Transforming_children_and_young_people_s_mental_health_provision.pdf
Department of Health & NHS England. (2015). Future in mind: Promoting, protecting and improving our children and young people’s mental health and wellbeing.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/414024/Childrens_Mental_Health.pdf
Dunnett, C. and Jones, M. (2020). Relational Policy and Practice. Relational learning – Support for schools and settings (devon.gov.uk)
Felitti, M. D., Anda, R. F., Nordenberg, M. D. et al (1998) ‘Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study’ American Journal of Preventative Medicine. 14.
Huppert, F.A. (2013). The state of wellbeing science. Interventions and Policies to Enhance Wellbeing: A Complete Reference Guide, Volume VI. John Wiley & Sons
Kumpfer, K. L. (2002). Factors and Processes Contributing to Resilience. IN Resilience and Development, pp. 179-224.
Lereya, T., & Deighton, J. (2019). Learning from Head Start: the relationship between mental health and school attainment, attendance and exclusions in young people aged 11 to 14. London: EBPU. https://www.ucl.ac.uk/evidence-based-practice-unit/sites/evidence-based-practice-unit/files/headstart_evidence_briefing_3.pdf
MacBeath, J. (2006). Finding a voice; Finding Self. Educational Review. 58. (2). 195 – 207.
Masten, A. S.(2001) Ordinary magic: Resilience processes in development. American Psychologist, 56, 227-238.
MIND, (2016). Mental Wellbeing. https://www.mind.org.uk/media-a/3360/mental-wellbeing-2016-pdf-version.pdf
NHS (2018). Mental Health of Children and Young People in England, 2017; A summary of key findings. https://files.digital.nhs.uk/A6/EA7D58/MHCYP%202017%20Summary.pdf
National Institute for Health and Care Excellence (NICE). 2019. Social and Emotional Wellbeing in Primary and Secondary Education Draft Scope for Consultation. NICE. https://www.nice.org.uk/guidance/GID-NG10125/documents/draft-scope
OFSTED (2019). The Education Inspection Framework.
Peterson, C. (2009). Positive Psychology. Reclaiming Children and Youth, 18(2), 3-7.
Pupil Participation: a best practice guide, (2016).
Rutter, M. 1979. Protective factors in children’s responses to stress and disadvantage. Annuals of the Academy of Medicine, Singapore, 8, 324-338.
Seligman, M. (2011). Flourish: A visionary new understanding of happiness and well-being. New York, USA: Free Press.
Treisman, K. (2018). The Therapeutic Treasure Deck of Grounding, Soothing, Coping and Regulating Cards. Jessica Kingsley Publishers.
World Health Organization, (2014). Definition of Mental Health.
United Nations Convention on the Rights of the Child. (1989). https://www.ohchr.org/en/professionalinterest/pages/crc.aspx
Veekan, J. (2012) Bear Feelings Cards. 2nd Edition. Q Cards.
Weare, K. (2015). What works in promoting social and emotional wellbeing and responding to mental health problems in schools. National Children’s Bureau.
https://www.ncb.org.uk/sites/default/files/uploads/documents/Health_wellbeing_docs/ncb_framework_for_promoting_well-being_and_responding_to_mental_health_in_schools.pdf
16. Appendix
16.1. Interactive factors framework template
16.2. Interactive factors framework: example
Authors
This document was produced by our Educational Psychology Service and SEMH Advisory teams. The authors include:
Dr Rachel Edmundson – Educational Psychologist
Claire Hoskin – Educational Psychologist
Dr Dan Nichols – Educational Psychologist
Dr Kirsty Hughes – Educational Psychologist
Conrad King – Educational Psychologist
Dr Rachel Hearn – Senior Educational Psychologist
Anthony Boulton – SEMH Team Lead
Bronwen Cox – Principal Educational Psychologist
This document was updated in October 2022 by Devon Educational Psychology Service.
We would also like to thank the Head teachers of Denbury Primary, Marwood and Education South West for their support and input and our colleagues in CAMHS, Public Health and School Nursing for their expertise and advice.
If you have any questions or would like to know more about our current offer, please contact:
Dr Dan Nicholls; Senior Educational Psychologist – Dan.nicholls@devon.gov.uk
or
Dr Rachel Hearn; Deputy Principal Educational Psychologist – Rachel.hearn@devon.gov.uk