Contents
Introduction – the facts
Poor emotional and mental health affects a significant number of children and young people:
- 1 in 10 children have a diagnosable mental health disorder; around 3 children in every classroom (i)
- 1 in 5 young adults have a diagnosable mental health disorder(ii)
- Half of all mental health problems manifest by the age of 14, with 75% by age 24 (iii)
- Almost 1 in 4 children and young people show some evidence of mental ill health (including anxiety and depression).
There is a substantial body of research evidence to suggest that young people’s social emotional and mental health (SEMH)needs have a significant impact on all aspects of their life including their learning and progress through the curriculum, behaviour in school and attendance, further training and employment and general life chances. Social media and new technology is also linked to increasing risks of poor SEMH.
In Devon, the number of exclusions has risen and SEMH is now the main category of need in SEN support. Children with identified special educational needs accounted for around half of all permanent exclusions and fixed term exclusions in Devon in 2016/17. It is therefore crucial that schools play a key role in understanding and supporting children’s social, emotional and mental health needs.
In order to promote inclusion and reduce exclusions, schools should employ a graduated response to meeting children and young people’s SEMH needs. This starts with a whole school approach and ethos in understanding and supporting social, emotional and mental health and engagement with parents and the community. It includes quality first teaching for all students ranging to targeted interventions for groups of pupils or individuals and lastly specialist interventions for those with the most complex needs.
The interventions in this Toolkit have been grouped into Universal, Targeted and Specialist to support schools to follow a graduated approach to SEMH and to identify the correct level of intervention based on need.
- Universal interventions are for all students
- Targeted interventions are for some students
- Specialist interventions are for a few students.
i. Green H et al (2005) Mental health of children and young people in Great Britain, 2004. Basingstoke: Palgrave MacMillan.
ii. Green H et al (2005) Mental health of children and young people in Great Britain, 2004. Basingstoke: Palgrave MacMillan.
iii.Kessler RC et al. (2005). ‘Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication’.
Universal evidence-based interventions: for all CYP with SEMH needs
Coaching
Coaching is a method that can be used to support school staff to develop their practice by providing an opportunity to set goals and work towards achieving them. Coaching can be carried out with a member of school staff by an outside professional (for example, an Educational Psychologist) or can be carried out between colleagues. There are many similarities between coaching and mentoring, which is also frequently used in schools to develop practice, however there are some key characteristics to coaching that make the process different.
Coaching uses a focused model to structure each session. There are a number of different models used by coaches, however these generally follow a similar routine of supporting the ‘coachee’ to identify what is currently working well, and the skills that they already possess. The session will typically also involve supporting the coachee to identify areas of their practice they would like to improve, or skills they would like to develop further, and setting these as outcomes.
Whereas other support processes such as mentoring, involve passing on knowledge and experience and offering solutions to problems, coaching instead relies on supporting the coachee to identify their own solutions and answers. The process typically consists of a number of regular sessions between the coach and coachee, where progress is discussed and new outcomes and targets set as needed.
Key area of need
Supporting members of school staff to reflect on and develop their own practice.
Age group
Teachers/school staff supporting any age group.
Where can I access information about this?
Educational Psychology Service
Evidence base
Existing research has highlighted that participation in coaching within education can lead to increased teacher wellbeing, reduced stress and increased resiliency skills, improved practice and improved leadership and performance management.
Limitations to research evidence
Although coaching has been used extensively in many settings, the use of coaching in educational settings is relatively new, and therefore the research in this area is emerging. As coaching is unique to the individual, it can be difficult to compare the experiences of individuals involved in the coaching process, and so research is generally qualitative and based on the self-reporting of participants.
Research references
Adams, M. (2015) Coaching Psychology in Schools: Enhancing Performance, Development and Wellbeing, Abingdon: Routledge.
Adams, M. (2016) ‘Coaching psychology: An approach to practice for educational psychologists’, Educational Psychology in Practice,32 (3), pp. 231-244.
Tolhurst, J. (2010) The Essential Guide to Coaching and Mentoring (2nded.), UK: Pearson Education.
Mindfulness
Mindfulness means knowing directly what is going on inside and outside ourselves, moment by moment. The idea of mindfulness is rooted in Buddhist traditions and was developed in the west largely by the work of Jon Kabat-Zinn, who developed Mindfulness-Based Stress Reduction (MBSR) programs at the University of Massachusetts Medical School in 1979. His work focused on helping patients deal with chronic pain.
Mindfulness approaches have since in developed in many areas of psychology including cognitive/behavioural approaches, neuroscience, positive psychology and emotion focused approaches. Mindfulness interventions involve attending to the present moment without judgement or attachment to any particular outcome. The aim of mindfulness is to learn to be aware of thoughts and bodily sensations in order to be able to better cope with daily emotions and challenges.
There are a number of providers of mindfulness training for children and young people and school staff in the UK. The largest is the Mindfulness in Schools project (MiSP) for primary and secondary schools. MiSP train adults to teach mindfulness to secondary aged pupils (.becourse) and primary pupils (pawsbe course). They also provide online and foundation level mindfulness training for school staff to understand the main principles of mindfulness. School staff need to be well trained and to continue to practise mindfulness themselves before teaching it to their students. Regular supervision and on-going professional development is also recommended.
Key area of need
Beneficial for all children; can promote resilience, self-awareness, empathy, attention, self-control and compassion.
Particularly useful for children with SEMH needs including anxiety, depression, behaviour difficulties.
Age group
All ages groups
Useful links to research
Where can I access information about this?
Educational Psychology Service
https://mindfulnessinschools.org
Evidence base
Katherine Weare undertook a systematic review of the research evidence into Mindfulness based interventions in schools in February 2018. The research indicates that mindfulness is a popular intervention with little adverse effects. Mindfulness based interventions can reliably impact in a wide range of indicators of positive psychological, social and physical wellbeing in children and young people. Mindfulness based interventions have small to medium positive impact on depression and emotional self-regulation and small positive effects on anxiety (Weare, 2018)
Limitations to research evidence
The research in this area is still in its infancy and a greater focus is needed to measure the impact of mindfulness on behaviour, academic performance and physical health.
Research references
Bluth, K., Campo, R. A., Pruteanu-Malinici, S., Reams, A., Mullarkey, M., and Broderick, P. C. (2015). ‘A school-based mindfulness pilot study for ethnically diverse at-risk adolescents.’ Mindfulness.
Kallapiran, K., Koo, S., Kirubakaran, R., and Hancock, K. (2015). ‘Effectiveness of mindfulness in improving mental health symptoms of children and adolescents: A meta-analysis’. Child and Adolescent Mental Health, 20: 182–194.
Kuyken, W., Weare, K., Ukoumunne, O. C., Vicary, R., Motton, N., Burnett, R., and Huppert, F. (2013). ‘Effectiveness of the mindfulness in schools programme: Non-randomised controlled feasibility study. The British Journal of Psychiatry, 203(2): 126–131.
Weare, K. (2015). ‘Evidence for mindfulness: impacts on the wellbeing and performance of school staff’. http://mindfulnessinschools.org/wp-content/uploads/2014/10/Evidence-for-Mindfulness-Impact-on-school-staff.pdf
Playfulness, Acceptance, Curiosity, Empathy (PACE)
An attitude of PACE – Playfulness, Acceptance, Curiosity, Empathy – aims to enable staff to engage with children and young people who have experienced neglect, abuse and trauma. PACE was developed by Dr Daniel Hughes (Clinical Psychologist) and research focused upon working with children and young people with attachment difficulties. The principles from PACE approaches aim to support the development of rapport and trust, and to help adults working with children and young people to build positive, secure relationships with them. These approaches are likely to be particularly relevant for adults working as key adults, teaching assistants or mentors for children with Social Emotional and Mental Health (SEMH)needs. PACE approaches are also often part of the training that foster carers and adoptive parents receive.
Dan Hughes has also developed Dyadic Developmental Psychotherapy (or DDP) Attachment Focused Treatment for Childhood Trauma and Abuse which is offered by some professionally trained therapists.
Key area of need
Social Emotional and Mental Health
Attachment difficulties
Relational needs
Age group
Appropriate for both Primary and Secondary age
Useful links to research or further information:
http://www.danielhughes.org/p.a.c.e..html
Where can I access information about this?
Educational Psychology Service
Evidence base
Dan Hughes has written a number of books regarding attachment and detailing how the principles of PACE can be used. Anecdotally it is reported that PACE approaches facilitate the emotional safety required to help children move from distrust of adults to trust and towards a more secure attachment.
Limitations to research evidence
There is limited research on the use of PACE principles in isolation as they tend to form part of wider interventions to support relational needs. However, the ideas from PACE have been widely shared and there is considerable practice-based evidence in terms of parents, staff and professionals finding them useful when considering their interactions with vulnerable children and young people.
Research references
Hughes, D.A. (2017). Dyadic Developmental Psychotherapy (DDP): An attachment-focused family treatment for developmental trauma. Australian & New Zealand Journal of Family Therapy; 38(4); p595-605.
Hughes, D.A. (2017) Building the Bonds of Attachment: Awakening Love in Deeply Traumatized Children. Third Edition. UK: Rowman & Littlefield Publishers.
Golding, K., & Hughes, D.A., (2012). Creating Loving Attachments: Parenting with PACE to Nurture Confidence and Security in the Troubled Child.UK: Jessica Kingsley Publishers.
Restorative approaches
A restorative approach in schools helps develop a healthier learning environment, where children and young people take responsibility over their own behaviour and learning. Restorative approaches enable those who have been harmed to convey the impact of the harm to those responsible, and for those responsible to acknowledge this impact and take steps to put it right.
Restorative approaches in schools focus on strengthening and repairing relationships, listening with empathy, valuing young people’s opinions and being curious about what has happened. In avoiding attributing blame but encouraging insight and taking responsibility for their actions, young people are supported to develop pro-social behaviour to repair harm and develop positive relationships.
Restorative approaches aim to:
- develop emotional literacy, responsibility and empathy
- create a more positive learning environment with better attendance, and fewer behaviour incidents
- raise children and young people’s awareness of the impact of their choices on others
- reduce the number of exclusions and help young people remain in mainstream education
To be effective, restorative approaches must be in place across the school. This means all pupils; staff (including non-teaching staff), management and the wider school community must understand what acting restoratively means and how they can do it.
Key area of need
Children and young people with emotional and social needs who often are involved in misunderstandings or conflicts with their peers or the adults supporting them
Age group
All ages
Where can I access information about this?
Educational Psychology Service
SEMH team
Evidence base
Research indicates that Restorative approaches can:
- increase attendance and reduce exclusions
- prevent bullying and respond to bullying effectively
- increase the confidence of school staff to deal with bullying and conflict
- build a culture of respect and discipline within a school
For example, the DfE (2010) survey 283 schools and found that 97% of schools felt that restorative justice reduced bullying. The majority of schools also reported that this approach was cost effective and easy to implement.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/182421/DFE-RR098.pdf
Limitations to research evidence
There is a wide range of restorative approaches and methods of implementation meaning that generalisation of research findings can be inappropriate and positive findings maybe context specific.
Research references
Department of Education (2010) The use and effectiveness of anti-bullying strategies in Schools. Thompson, F. & Smith, P.K. DfE
Hopkins, B. (2011) The Restorative Classroom: Using Restorative Approaches to Foster Effective Learning. Speechmark.
Mahaffey, H. & Newton, C. (2008) Restorative Solutions: Making it work. Inclusive Solutions UK Ltd
Social and Emotional Aspects of Learning (SEAL)
SEAL is a comprehensive universal whole school approach to developing social and emotional skills in all children. It is a curriculum resource which aims to develop social and emotional aspects of learning focusing on five key qualities/skills: self-awareness, managing feelings, motivation, empathy and social skills. These skills underpin positive behaviour and promote effective learning. SEAL also aims to increase attendance rates, staff effectiveness and the emotional well-being of the staff and pupils in schools. This resource has been very popular nationally and historically has been used in most schools across the UK. Whilst the resources have been archived by the DfE they are still available online from a number of sources.
Key area of need
All children.
Age group
Foundation stage through to secondary.
Where can I access information about this?
Educational Psychology Service
SEMH team
Evidence base
In primary schools SEAL has been shown to have a positive impact on both pupils and staff. In regard to pupils, the research indicates that it can improve children’s confidence, social skills, conflict resolution, behaviour in the classroom and on the playground, and ability to communicate and manage emotions. Some research also indicates a reduction in bullying type behaviours. In regard to impact on school staff, SEAL has been shown to increase staff confidence when managing pupils’ behaviour and increase understanding of social and emotional needs.
Evaluations of SEAL in secondary schools are less positive and the authors of these studies have hypothesised that this may be linked to secondary schools finding it more difficult to embed new whole school approaches and interventions. When SEAL was not carefully implemented, there were no positive impacts upon pupil’s social and emotional skills, or pro-social behaviour.
Limitations to research evidence
There are difficulties comparing results between schools using SEAL as schools varied in the extent to which they were implementing the SEAL curriculum. Most studies lacked a control group so outcomes cannot necessarily be attributed to SEAL intervention.
Research references
Humphrey, N., Lendrum, A., & Wigelsworth, M. (2010). Social and emotional aspects of learning (SEAL) programme in secondary schools: National evaluation. Manchester: DfE.
Humphrey, N., Lendrum, A., & Wigelsworth, M. (2013). Making the most out of school-based prevention: Lessons from the social and emotional aspects of learning (SEAL) programme. Emotional and Behavioural Difficulties,18(3), 248-260.
Lendrum, A., Humphrey, N., & Wigelsworth, M. (2013). Social and emotional aspects of learning (SEAL) for secondary schools: implementation difficulties and their implications for school‐based mental health promotion. Child and Adolescent Mental Health, 18(3), 158-164.
Wigelsworth, M., Humphrey, N., & Lendrum, A. (2012). A national evaluation of the impact of the secondary social and emotional aspects of learning (SEAL) programme. Educational Psychology, 32(2), 213-238.
The Thrive Approach
The Thrive Approach is an intervention based on principles of neuroscience, attachment theory and child development in order to promote the social and emotional development of children and young people.
The Thrive Approach provides a model of development comprised of a number of stages that children and young people are expected to progress through. The model then offers a range of play-based and creative activities that can be used to support children to progress through these stages and to identify any gaps or missed experiences that can then be addressed.
The Thrive Approach also offers an online tool, Thrive-Online, which is an essential part of the approach. This is accessed through a subscription to the service. Thrive-Online can be used to assess an individual’s level of social and emotional development, and then to identify the support they are likely to require. Thrive-Online can be used with individuals but can also be used to ‘profile’ larger groups.
Key area of need
General social and emotional needs, as well as increasing adult understanding.
Age group
Both primary and secondary students.
Where can I access information about this?
Please see https://www.thriveapproach.com for more information.
Useful links to research
Evidence base
The Thrive Approach website offers a range of research evidence supporting the theoretical underpinning of the Thrive model, however there is no published research evaluating the impact of the Thrive Approach on children and young people. There are a number of case studies available on the Thrive website. Unpublished research carried out by an Educational Psychologist as part of their doctoral training identified that the Thrive Approach did not have a significant positive impact on pupils in terms of outcomes measured (sense of relatedness, emotional reactivity and readiness to learn).
Limitations to research evidence
There is very little published evidence available on the Thrive Approach at present.
Research references
Cole, M. (2012) ‘Promoting emotional wellbeing and inclusion for children identified with Emotional and Behavioural Difficulties in mainstream primary schools: an evaluation of a psychotherapeutic approach (Thrive)’, Unpublished doctoral thesis.
Howarth, K. (2013) ‘Thrive training and Thrive trainees’ perceived relationships with children with BESD, self-efficacy in managing children’s BESD and causal attributions about BESD in children: a two-phase evaluation’ Unpublished doctoral thesis.
Targeted evidenced based interventions: for some CYP with SEMH needs
Attachment based mentoring
The Attachment Based Mentoring project was born out of concerns regarding the achievement and inclusion of children in care and children in need in Devon. Research and statistics indicate that life chances and outcomes for these groups are significantly lower than their peers. They struggle to engage with learning and are at great risk of mental health difficulties and of exclusion from school.
Attachment based mentoring was developed to provide a different kind of support, to enable children to connect with the education on offer. It seeks to address the child’s primary social, emotional and mental health needs which then enables the child to access the learning and social environment and develop greater resilience.
The model of mentoring drawing on research from attachment theory, solution focused coaching, social learning theory and resiliency and has three components: ‘Attachment and Relationships’, ‘Development’ and ‘Practical Support’, with the mentor acting as significant adult, coach and parent in school.
School staff are trained to meet the specific needs of children in care and other vulnerable children, by providing them with a significant adult in school who is able to use coaching and mentoring to support their development. Whilst all children being mentored will have personalised outcomes, intended impact is that children will:
- develop their feelings of security, resilience and general wellbeing
- develop the ability to regulate their emotions and behaviour
- reach their academic potential
- be fully included in school
This intervention has been very successful in Devon. Between 2016 and 2018, 240 mainstream school staff were trained and over 300 special school staff. These staff have also received follow up supervision.
Key area of need
Children in care and adopted children.
Children with attachment difficulties and/or known to Social Care.
Age group
From Early Years through to secondary aged pupils.
Where can I access information about this?
Educational Psychology Service
SEMH team
Evidence base
Evaluation of the Attachment Based Mentoring project between 2016-2018indicates that the mentoring is having a positive impact in several areas.
- School staff working with the children (both teachers and mentors) commented that the mentoring had a positive impact on the children’s ability to be open and trusting.
- School staff noticed increased feelings of self-worth, confidence and happiness in children being mentored. This manifested itself in a greater ability to reflect on behaviour, take responsibility and to understand and regulate their emotions. These are strong indications that providing a significant adult for the children in school is supporting them to develop a greater sense of security and belonging and a healthy self-esteem.
- Teachers reported increased ability to concentrate, ask for help, accept challenges and admit mistakes, work with others and take part have most commonly been reported.
Limitations to research evidence
This project has only been delivered and rolled out in Devon and has not been evaluated further afield or in a different geographical context.
Circle of Adults
Supporting staff in problem-solving around challenging behaviour: Circle of Adults is a meeting where all relevant professionals can discuss issues, experiences, and concerns with a view to joint problem solving. What is said in the meeting can be kept confidential and solutions can be fed back to parents and the young person themselves at a later date.
Firstly, the problem should be discussed and everyone given a chance to share their thoughts. It is important to recognise that the child/young person is struggling with a problem and that the child/young person is not the problem. Hypotheses and solutions should be kept for later on in the meeting. It is useful to set a time limit i.e. 1.5 hrs. Information should be recorded using the X Mind software or large graphic facilitation as below and then it can be distributed to all members of the group.
There are 8 sections that are explored and represented graphically
- Ground rules (respect, confidentiality, sensitive language, empathy, listening)
- Presenting problem: a rich picture of pupils’ behaviour, circumstances, difficulties
- Child/Young person’s viewpoint (represented by an adult present) developing empathy
- Helpful metaphors (walking on eggshells, Jekyll and Hyde, Firework etc.)
- Exploring relationships, (school family, friends, wider community)
- Organisational Factors (helpful vs hindrance)
- Hypotheses (what’s happening?)
- Strategies (including First Steps to start immediately)
Key area of need
Pupils with social, emotional difficulties which result in challenging behaviour or poor emotional wellbeing.
Age group
Pupils may be from Key stages 2-4. Sessions last for 90 minutes and require a minimum of six and a maximum of 12 staff members, including the case presenter
Where can I access information about this?
Educational Psychology Service https://www.devon.gov.uk/support-schools-settings/send/educational-psychology/educational-psychology-service/
Circle of Friends
The Circle of Friends approach seeks to develop a support network around individuals in the school community who are experiencing social difficulties. School staff seek out volunteers from the child or young person’s peer group who are willing to support the child or young person who is felt to be struggling with social situations. The group meets regularly with the member of staff to problem solve with the target pupil in order to address any social difficulties that he/she may be experiencing in school.
There are different ways in which a Circle of Friends can be set up. It can vary in terms of whether the target child is not present at the initial class discussion or whether, as in the adapted version described by Barratt and Randall (2004) the focus child is never singled out from the peer group and is present at the initial class discussion with the intervention introduced as a way of helping those involved to get to know one another more and become better friends.
Key area of need
Social skills and friendships
Social isolation
Age group
This intervention can be adapted for Primary or Secondary age pupils. The form of the group, how participants are selected and their ongoing engagement needs careful consideration.
Where can I access information about this?
Educational Psychology Service
SEMH team
Evidence base
There have been a number of studies that have suggested positive benefits in peer relationships and social skills for children and young people participating in this approach.
Limitations to research evidence
The results from research studies have varied in terms of measurable outcomes. The study by Fredrickson & Turner (2003) found few changes on other measures of perceptions or behaviour other than social acceptance. The impact of the approach is likely to be affected by factors such as teacher attitudes, classroom climate and whole school ethos (Taylor & Burden, 2000).
Research references
Barrett, W., & Randall, L. (2004). Investigating the Circle of Friends Approach: Adaptations and implications for practice. Educational Psychology in Practice, 2004.
Frederickson, N., & Turner, J. (2003) Utilizing the Classroom Peer Group to Address Children’s Social Needs: An Evaluation of the Circle of Friends Intervention Approach. Journal of Special Education 36(4).pp.234-245
James, A., & Leyden, G. (2010). Putting the Circle back into Circle of Friends: A grounded theory study. Educational & Child Psychology, 27(1), pp.52-63.
Emotion coaching
Emotion coaching is based on the understanding that all behaviour is a form of communication and is driven by an emotional response. Based on research by American Psychologist John Gottman, Emotion Coaching uses moments of heightened emotion and resulting behaviour to guide and teach the child and young person about more effective responses. Through empathetic engagement, the child’s emotional state is verbally acknowledged and validated, promoting a sense of security and feeling ‘felt’. This activates changes in the child’s neurological system and allows the child to calm down, physiologically and psychologically. Inappropriate behaviours are addressed when the child is calmer and the child is supported to problem solve and engage in solution-focused strategies. Emotion coaching provides a staged approach to developing scripts of how to respond to pupil’s when their emotions become overwhelming.
Key area of need
Emotional literacy – ability to express emotions
Changing behaviour and developing problem solving
Age group
This is suitable for all age groups from early years to secondary. This approach can be used by all adults working with children and young people.
Useful links to research
Where can I access information about this?
Educational Psychology Service
https://www.emotioncoachinguk.com
Evidence base
Research from America and Australia suggests that Emotion Coaching has a positive impact on children and young people’s SEMH (including depression and conduct difficulties), academic achievement and resilience when exposed to abuse and violence (Gottman et al, 96). It has been used to effectively support children to overcome trauma and reduce externalising behaviours in children with Autism. It is positively correlated with secure attachments.
UK research is emerging. Bath Spa University is currently working in partnership with Somerset County Council’s Children and Young People Health and Wellbeing in Learning Programme to deliver a programme of Emotion Coaching training to the children and young people’s workforce across the five districts of Somerset. Recent evaluations of the project have found increased empathetic awareness and ability to label communicate emotions, improved self-regulation and well-being and increased enjoyment and engagement in children and young people in early years, primary and secondary settings. https://www.bathspa.ac.uk/media/bathspaacuk/education-/research/attachment-aware/Emotion-Coaching-Executive-Summary-2017-(1).pdf
Limitations to research evidence
Research regarding the impact of emotion coaching when used in education settings in the UK is limited and currently there is no longitudinal information.
Research references
Chen, F.M., Lin, H.S.& Li, C.H. (2012). The role of emotion in parent-child relationships: Children’s emotionality, maternal meta-emotion, and children’s attachment security. Journal of Child and Family Studies, 21(3), 403–410.
Gottman, J.M., Katz, L.F. & Hooven, C. (1996) Parental meta-emotion philosophy and the emotional life of families: Theoretical models and preliminary data. Journal of Family Psychology, 10(3), 243–268.
Gus, L., Rose, J. & Gilbert, L. (2015) Emotion Coaching: a universal strategy for supporting and promoting sustainable emotional and behavioural well-being, Educational and Child Psychology,32(1), 31-41
Katz, L.F., Hunter, E.& Klowden, A. (2008). Intimate partner violence and children’s reaction to peer provocation: The moderating role of emotion coaching. Journal of Family Psychology, 22(4), 614–621.
Wilson, B.J., Berg, J.L., Zurawski, M.E. & King, K.A. (2013). Autism and externalising behaviours: Buffering effects of parental emotion coaching. Research in Autism Spectrum Disorders, 7(6), 767–776
Emotional Literacy Support Assistants (ELSA)
The ELSA project is a national initiative developed by Sheila Burton, Educational Psychologist, to build the capacity of schools to support the emotional needs of their pupils from within their own resources. It recognises that social, emotional and mental health underpins learning and pupil well-being and that children learn better and are happier in school if their emotional needs are also addressed.
Educational Psychologists train teaching assistants to become ELSAs and provide them with ongoing supervision from educational psychologists. There is also a nation network of support. Please see https://www.elsanetwork.org.
ELSAs work with pupils individually or in small groups in order to develop their emotional literacy skills. ELSAs are trained to support pupils in the following ways:
- Managing emotions including anger and anxiety
- Social and friendship skills
- Using social and therapeutic stories
- Loss, bereavement and family break up
- Active listening and reflective conversation skills including working with puppets
The ELSA training programme has been running in Devon since 2016 and staff from over 50 schools have been trained as ELSAs. The 16/17 evaluation of the ELSA programme in Devon found that as a result of the ELSA training, teaching assistants had a better understanding of emotional literacy and how it affected pupil’s learning. They also felt more confident using active listening and reflective conversation skills.
Key area of need
Social, emotional and mental health
Difficulties with peers and relationships
Self-esteem and confidence
Challenging behaviours
Age group
From Early Years through to secondary aged pupils.
Where can I access information about this?
Educational Psychology Service
https://www.devon.gov.uk/support-schools-settings/send/educational-psychology/educational-psychology-service/
The ELSA Network
Useful links to research
Evidence base
ELSA is becoming increasingly popular around the UK and growing numbers of Educational Psychologists have delivered and evaluated the training programme. Research has found that ELSA intervention has a positive impact on the support provided for emotional wellbeing throughout the whole school. Research suggests that ELSA has a positive impact on attendance, academic attainment and concentration. It also supports children and young people to be resilient and to manage transition. Some studies have shown a reduction in bullying.
In regard to the positive impact on individual pupils, ELSA is credited with supporting the following skills:
- empathy, self-awareness, and self-regulation, self-esteem
- improved social behaviour and friendships
- decrease in behaviours that cause concern including hyperactivity and conduct problems
- increase in positive behaviours such as asking for help)
Research suggests that ELSA training and intervention also has a positive impact on school staff by increasing the knowledge and confidence of school staff to support the emotional needs of pupils.
Limitations to research evidence
Research in this area is still developing and not all research is published in peer review journals. Research by EPs for their own services could be subject to bias and is not truly independent. There is no longitudinal research at this stage to suggest long term benefits of ELSA.
Research references
Burton, S., Osborne, C., & Norgate, R. (2010). An evaluation of the impact of the Emotional Literacy Support Assistant (ELSA) project on pupils attending schools in Bridgend. Hampshire Educational Psychology Service, Research & Evaluation Unit.
Hill, T., O’Hare, D. & Weidberg, F. (2014) “He’s always there when I need him”: Exploring the perceived positive impact of the Emotional Literacy Support Assistant (ELSA) programme. Bristol University.
Mann, D. (2014). A mixed methods evaluation of the Emotional Literacy Support Assistants (ELSA) project. University of Nottingham.
Miles, N. (2014). An Exploration of the Perceptions of Emotional Literacy Support Assistants (ELSA) of the ELSA-Pupil Relationship. Cardiff University.
Partt, K., & Mann, F. (2015). ELSA Evaluation Report December 2015. Support Services for Education, Somerset.
The Homunculi Approach to Social and Emotional Wellbeing
The Homunculi Approach is described as a flexible Cognitive Behavioural Therapy programme for young people on the autism spectrum or with emotional and behavioural difficulties. It seeks to build social and emotional resilience in children and young people. It is designed as a 10 week programme that teaching staff (or parents) could use with a child or young person. The materials in the book and the programme have been designed to be used by anyone, without the need for a background in therapeutic approaches. Homunculi is a Latin word meaning ‘little people’. The Homunculi characters are miniature agents with problem solving missions which the child or young person is supported to create, linked to the problems that the child or young person wants to solve. It is designed to be used individually or as a group intervention and with a level of personalisation in line with the interests of the target pupils.
Key area of need
Trouble identifying emotions and negotiating social situations.
Autism Spectrum Condition, suggested to be particularly well suited to those with high functioning autism (what was previously referred to as Asperger’s syndrome).
Age group
Designed for children from seven years old upwards.
Where can I access information about this?
Educational Psychology Service
Evidence base
Within the text, the authors of the programme detail positive results from a case study with a 13 year old young man with a diagnosis of Asperger’s Syndrome (Greig and MacKay, 2005) and a further research study involving over 30 young people (MacKay & Greig, 2008) who had variety of special needs, with only half of the sample having a diagnosis of ASC. The authors suggest benefits on a range of self-ratings for a range of specific issues including exam stress, friendship problems, low self-esteem, coping with change, and anxiety. This second study suggests that whilst The Homunculi was designed for children and young people with ASC it may be helpful for those with a variety of difficulties including SEMH.
Limitations to research evidence
As a relatively new approach there is not yet an established evidence base considering the impact of the approach when implemented by school staff using the resource text. The research below is based upon the work of the authors of the programme.
Research references
Greig, A. & MacKay, T. (2005). Asperger’s Syndrome and cognitive behaviour therapy: New applications for educational psychologists. Educational and Child Psychology, 22(4), pp.4-15.
MacKay, T. & Greig, A. (2008) The Homunculi: A cognitive behaviour therapy programme for young people with autistic spectrum disorders and other difficulties. The British Psychological Society Annual Conference 2008 Book of Abstracts, pp.161-162. Leicester, UK: British Psychological Society
Menzies, D. (2014). The Homunculi approach to social and emotional wellbeing: a flexible CBT programme for young people on the autism spectrum or with emotional and behavioural difficulties. Educational Psychology in Practice, 30(2), pp.215-216.
MAPs (Making Action Plans)
A team approach to person-centred planning in order to support young people to identify goals. MAPs is an 8-step process that guides the group from the ‘story so far’ through to positive action planning to work towards the child or young person’s identified dreams, goals and wishes.
MAPs is a Person-Centred Planning approach aimed at creating a shared vision of a positive future for the individual and their family. It provides a space for discussing different possible futures for the individual and how these can be planned for using their individual strengths, gifts and talents. MAPs can be used to support children or young people when entering a new school, leaving school, or when coping with a loss or dealing with a difficult time in life. There are times when life’s changes call for new responses and it is good for the young person to re-tell their story in order to affirm their gifts and make action agreements that will lead to better opportunities.
The process is co-facilitated by two Educational Psychologists, in the roles of ‘Process’ and ‘Graphic Facilitator’, who work together to effectively manage the process through each of the six steps. It is seldom that they contribute directly to the content of the session. The ‘Graphic Facilitator’ keeps a graphic record of each step of the process, capturing the essence of what has been said at each step. This graphic summary remains the property of the young person. The school are also provided with an electronic copy of the visual summary.
The process takes 2 hours, consisting of 90 minutes for the group process, plus 30 minutes for administration. Those who attend will need to commit to staying for the full 90 minutes until the process is completed.
Who does it involve:
- a young person who requires support with identifying new goals, and the actions required to achieve those goals
- a supportive group of problem solvers (4-12 people), who have been identified by the young person as key people who can help them to achieve their identified goals, often consisting of the young person’s friends, family, and other professionals and support workers who know the young person well
- two Educational Psychologists, in the roles of ‘Process Facilitator’ and ‘Graphic Facilitator’
Key area of need
SEMH
Age Group
Ages 10-18 years
Useful links to research
http://www.inclusive-solutions.com
Where can I access information about this?
Educational Psychology Service
Motivational interviewing
Motivational Interviewing is a method of positive behaviour management which is achieved by active reflective listening to the pupil. Showing Unconditional Positive Regard (verbal and non-verbal) is central to motivational interviewing. Communicating to the pupil that what they say is important, they are worth listening to and they are valued are the key elements of motivational interviewing. Reflecting back what the pupil says (using pupil’s own words and phrases) to elicit further thoughts and feelings and summarising, structuring and selectively guiding the pupil helps them to gain insight into their own behaviour.
Therefore, pupils are more likely to feel supported and have the motivation to decide to change their behaviour. The pupil builds their motivation by feeling heard and the success of any self-management programme is dependent on the pupil wanting to change his/her own behaviour.
The stages of change model by Prochaska and Di Clemente (1983) can be used as part of Motivational Interviewing.
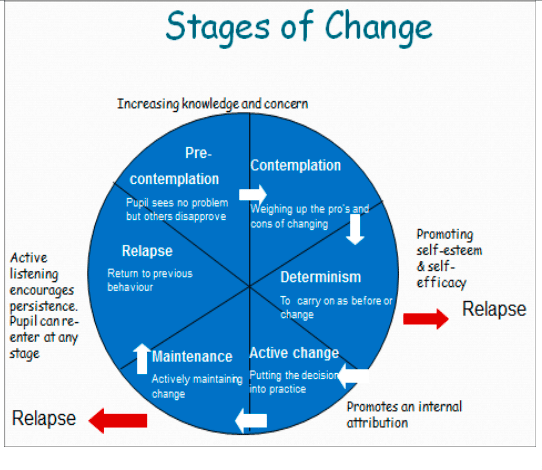
- At the Pre-contemplation and Contemplation stages active listening promotes knowledge and concern.
- At the Determinism stage active listening promotes self-esteem and self-efficacy.
- The Active Change stage promotes an internal attribution that increases the belief that the ‘problem’ can be influenced by the pupil’s efforts.
- If a Relapse occurs (and it most likely will!) then active reflective listening can encourage persistence and the stages of change may be re-entered at any appropriate stage
Miller and Rollnick, the originators of Motivational Interviewing, have redefined the approach to around three central elements:
- Spirit (acceptance, compassion, evocation and partnerships) which unpins the philosophy behind using Motivational Interviewing.
- Hierarchy of processes for working with clients is specified –engaging, focusing, evoking and planning
- Core skills, (defined by the acronym OARS) Open questions, Affirmations, Reflections and Summaries.
Key area of need
Changing behaviour for pupil’s own well being
Age group
Ages 10 years to adult
Useful links to research
Where can I access information about this?
Educational Psychology Service
Evidence base
Motivational Interviewing has been widely reviewed and found to be effective in medical research. In education, motivational interviewing has been used to successfully increase a young person’s motivation to change problematic behaviours or attitudes.
Limitations to research evidence
Motivational interviewing was a technique originally developed to help people struggling with addiction including alcoholism. Further research specifically about its impact in education settings is needed.
Research references
Atkinson C, Bragg J, Squires G, Muscutt J, Wasilewski D. Educational psychologists and therapeutic interventions: Preliminary findings from a UK-wide survey. Debate.2011;140:6-12.
Miller WR, Rollnick S. Motivational Interviewing, Third Edition: Helping People Change. New York: Guilford Press; 2012
Nuture groups
Nurture groups were initially developed by Marjorie Boxall in 1969, in order to immerse children in an accepting and warm environment, and to enable them to form positive relationships in school.
Nurture groups usually consist of between 6 and 12 pupils, usually supported by two members of staff. Children remain a part of their usual class but spend part of the school day in the nurture group setting. The amount of time spent in the nurture group is dependent on the needs identified, and this is usually done through the use of the Boxall Profile, an assessment tool which focuses on these areas.
Within the nurture group setting, there is a focus on six principles of nurture:
- learning is understood developmentally
- the classroom offers a safe base
- the importance of nurture for the development of wellbeing
- language is a vital means of communication
- all behaviour is communication
- the importance of transition in the lives of children and young people
(taken from the Nurture Group website, www.nurtureuk.org).
When pupils have met the targets identified through the Boxall profile, they reintegrate back into their usual class full time. Students typically access the nurture group intervention for between 1 and 4 terms.
Key area of need
Nurture groups generally support children with social and emotional needs, although also identify and attempt to reduce barriers to learning.
Age Group
From Early Years through to secondary aged pupils.
Where can I access more information about this?
Please see www.nurtureuk.org for more information.
A number of schools in Devon use the Nurture Group approach; however, there are currently no groups in Devon registered with the Nurture Group network.
Information on achieving accreditation and support to set up a group can be found on the Nurture Group website.
Useful links to research
Evidence base
The following quote regarding the evidence base for nurture groups is taken from the Nurture Groups website:
There are over 62 academic studies in the last two decades researching nurture group provision, including five non-randomised studies that have shown children and young people attending nurture groups are more likely to improve in social and emotional functioning than their peers that remain in the mainstream class.
Generally, Nurture Groups are found to have found positive impacts on the pupils attending them in terms of:
- improving skills for learning, including literacy and language skills
- improving pro-social skills and relationships with peers
- improvement in behaviour both in school and at home
These impacts were found to be more significant in younger children accessing nurture groups at an earlier age, and in those settings where nurture groups had been established for at least 2 years.
Limitations to research evidence
There is limited evidence looking at the longer-term impacts of nurture groups on those that have attended them. There is also limited research focused on the nurture group experiences of secondary school pupils, in comparison to early years and primary school pupils.
The Nurture Groups website also highlights that there is limited qualitative data looking at nurture groups where there is a large range of needs and behaviours, ages and genders within the group.
Research references
Griffiths, R., Stenner, R. and Hicks, U. (2014) ‘Hearing the unheard: Children’s constructions of their Nurture Group experiences’, Educational and Child Psychology, Vol. 31 (1).
MacKay, T.,Reynolds, S. & Kearney, M. (2010)‘From attachment to attainment: The impact of nurture groups on academic achievement’ Educational & Child Psychology, 27 (3).
O’Connor, T. &Colwell, J. (2002) ‘The effectiveness and rationale of the “nurture group” approach to helping children with emotional and behavioural difficulties remain within mainstream education’, British Journal of Special Education, 29 (2), pp.96–100.
Sanders,T.(2007) ‘Helping children thrive at school: The effectiveness of nurture groups’, Educational Psychology in Practice, 23 (1), pp. 45 –61.
Seth-Smith, F., Levi, N., Pratt, R.,Fonagy, P. & Jaffey, D. (2010) ‘Do nurture groups improve the social, emotional, and behavioural functioning of at risk children?’ Educational and Child Psychology, 27, (1)
Solution circles
‘Solution Circles’ is an evidence-based problem-solving approach: a group-based structured, six stage process, with each stage having a time allocation in order for the whole process to be complete in 30 minutes. Supportive challenge, reflective practice and personal support are threads that will run through the approaches used.
Solution Circles involve:
- One individual outlining a difficulty or feelings of being ‘stuck’, whilst the group listens.
- The group are then invited to ask clarification questions.
- Next the group are invited to generate and pose a range of solutions to the ‘Problem Presenter’ who must not respond!
- Then there is the opportunity for a group discussion, to explore and clarify with the ‘Problem Presenter’, which solutions brainstormed might be helpful and to discuss these further.
- The process then concludes with The First Step where the ‘Problem Presenter’ and the group decide on the first steps that are achievable within the next 3 days. It is crucial that at least one step is initiated within 24 hours.
- To finish, the group are asked for their final rounds of words to describe their experience. The ‘Graphic Recorder’ then provides the ‘Problem Presenter’ with the visual record of the discussion.
A session will also typically include:
- Check-in activities: noticing, acknowledging, sharing and hearing our thoughts and feelings and those of others.
- De-brief activity: involves noticing, acknowledging, sharing and hearing thoughts and feelings about the supervision session.
Key area of need
Solution circles provides an opportunity for staff to reflect on and review their practice, discuss individual children and young people’s needs in depth, explore how to change or modify their own practise, and gain emotional support for the challenges experienced. The benefits can include increased resilience with managing the demands of the role, whilst gaining ongoing professional development opportunities. This can be particularly useful when working with children and young people with complex and challenging needs.
Age group
Any age
Where can I access information about this?
Educational Psychology Service Inclusive Solutions – https://inclusive-solutions.com/circles/solution-circles
Staff supervision
Staff supervision can take numerous forms and is underpinned by a range of psychological theories and approaches, however, all approaches are founded on the idea of providing regular opportunities to review, reflect, evaluate and develop professional practice in a safe, supportive environment.
An overwhelming majority of the UK’s education professionals have suffered mental health issues as a result of their jobs (YouGov, Education Support Partnership, 2017). The pressures of audit and assessment mean that teachers often have relatively little time to meet and discuss new approaches to teaching and supporting students. A frequent criticism of the outsourcing of CPD is that trainers come in, do their training and then disappear; the training tends to be superficial (Weston, 2013).
Supervision offers a solution to this and the opportunity for staff to:
- reflect on and review their practice
- discuss individual children and young people’s needs in depth
- explore how to change or modify practice
- gain emotional support for challenges experienced Group supervision involves face-to-face meetings, on an agreed, regular basis.
Supervision can be in a group or on a one-to-one basis. In group supervision, the supervisor facilitates a specific process to enable individual staff to receive support from colleagues to analyse tricky or complex situations or issues, generating alternative solutions and providing supportive feedback. Each group supervision session requires supervisees to attend for 1½ hours.
Key area of need
For all staff working with children and young people
Age group
All ages
Where can I access information about this?
Educational Psychology Service – https://www.devon.gov.uk/support-schools-settings/send/educational-psychology/
Evidence base
In Devon, the Educational Psychology Service has been effectively running supervision groups for school staff. Informally, staff have reported that the supervision supports them to problem solve, gives them additional skills and knowledge, helps them to feel emotionally supported in their role and enhances well-being and better enables them to support the needs to challenging children and young people.
Limitations to research evidence
Much of the British research in this area is limited and outdated. Further research needs to be untaken
Research References
CWDC (2010). Inspiring practice. A guide to developing an integrated approach to supervision in Children’s Trusts. Leeds: CWDC.
Hawkins, P. and Shohet, R. (2007) Supervision in the helping professions (3rd ed.). Milton Keynes: Oxford University Press.
Scaife, J (2001). Supervision in the mental health professions: A practitioner’s guide. Hove: Routledge.
Specialist evidence-based interventions: for a few CYP with complex SEMH needs
From Timid to Tiger
From Timid to Tiger is a programme designed for parents of children with anxiety disorders. The text is described as an essential manual for mental health professionals who work with young anxious children and their parents. It is organised into a ten-session parenting–based course, which provides parents with simple cognitive behavioural techniques in a step-by-step approach for helping their children to manage their worries and fears.
The authors state that the book is aimed primarily at mental health professionals and suggest that to run a complete programme a core professional background in mental health is needed. They also suggest that at least one group leader needs some training and experience in cognitive behavioural therapy (CBT) and one in behaviourally based parent training programmes.
Key area of need
Anxiety
Age Group
Children under the age of 11years old. The authors state that it can be used with children as young as three years.
Useful links to research
Where can I access information about this?
Training is being offered by Early Help 4 Mental Health.
http://eh4mh.co.uk/from-timid-to-tiger/
Evidence base
The From Timid to Tiger manual states that it has been evaluated for use with children with a range of primary anxiety disorders, including separation anxiety, generalised anxiety, panic, agoraphobia and specific phobias. Cartwright-Hatton et al., (2011) detail significant reductions in anxiety for those children whose parent received the intervention.
Limitations to research evidence
The research into the impact of the programme is currently limited. The authors note that it has not been tested with children with a primary diagnosis of Post-Traumatic Stress disorder, although they state it has been used and shown to have benefits with a number of children who have been exposed to trauma. Likewise, if has not been evaluated for children with a primary diagnosis of obsessive compulsive disorder. The authors state that they have been deliberately relaxed about comorbid disorders as they state that many of the children they have worked with have had difficulties other than anxiety and appear to have done well in the programme.
Research references
Cartwright-Hatton, S., McNally, D., Field, A.P., Rust, S., Laskey, B., Dixon, C., Gallagher, B., Harrington, R.,Miller, C., Pemberton,K., Symes, W., White, C., Woodham, A.(2011)A new parenting-based group intervention for young anxious children: results of a randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry,50(3), pp.242-251
Lego-based therapy
Lego-Based Therapy is an intervention designed by Daniel LeGoff and his colleagues to promote social development in children using Lego as a resource. It was originally developed as an intervention for children with Autism Spectrum Conditions (ASC), however has successfully been used with other children with social communication difficulties.
The intervention involves children working collaboratively to create Lego models using a ‘barrier’ game approach. The children are encouraged to communicate, problem-solve and collaborate together to complete the model, with the support of an adult. The group can consist of 2+ pupils, each with their own specific role that focuses on a specific aspect of the model building. These roles can vary with the number of children in the group, and each pupil will get to experience each of the roles. The most basic roles for groups of 2 are as follows:
- Builder –The person that puts the bricks together.
- Parts supplier –They will find and give the bricks to the builder.
As the group becomes larger, further roles can be added including:
- Engineer – this person describes the bricks that are needed in terms of size, shape and colour.
Before working collaboratively with a peer, it is important to ensure that the child has developed the skills needed – they can identify and sort pieces according to shape, size and colour and can also describe these. The focus of the group can be adapted as needed, either following instructions to build a set model or ‘free building’ a model of the group’s choice.
Key area of need
Autism Spectrum Conditions (ASC) or other social communication difficulties.
Age group
There are no strict guidelines regarding the age group that Lego-Based Therapy is most appropriate for, as this depends on the child’s language skills (are they able to accurately describe and sort the bricks), the complexity of the models built and the children’s interest in Lego. It has successfully been used in both primary and secondary settings.
Where can I access this in Devon?
Communication and Interaction team Educational Psychology Service
Evidence base
Research published by Daniel LeGoff himself has suggested that during the course of the Lego-Based Therapy intervention, there were significant improvements in participants’ ability to initiate social contact with peers, sustain interaction with peers and overcome aloofness and rigidity. These improvements were found both after 12 and 24 weeks.
Research carried out by an Educational Psychologist as part of doctoral training suggested that children found the groups enjoyable and found working with others and forming new friendships motivating. However, many preferred building by themselves and could become frustrated with their peers during the group.
Limitations to research evidence
There is a limited amount of independent research that has been published regarding the efficacy of Lego-Based Therapy interventions. Whilst some qualitative research exists, there is limited data examining progress made during the sessions.
Research references
Brett, E. (2013) LEGO Therapy: Developing Social Competence in Children with Asperger Syndrome through Collaborative LEGO Play, Unpublished Doctoral Thesis.
LeGoff, D., Gomez de la Cuesta, G., Krauss, GW and Baron-Cohen, S. (2014) Lego-Based Therapy How to build social competence through LEGO-Based Clubs for children with autism and related conditions, Philadelphia: Jessica Kingsley Publishers.
The Overcoming Programme
The Group Overcoming Programme is a guided Cognitive-Behavioural Therapy (CBT) programme for parents of anxious children. It can be used to support children with a range of anxiety disorders including separation anxiety disorder; social phobia; specific phobia; generalised anxiety disorder; and agoraphobia/panic. Questionnaire measures, such as The Spence Child Anxiety Scale (SCAS; Spence, 1998) or The Revised Child Anxiety and Depression Scale (RCADS; Chorpita et al., 2000) should be used to aid assessment and appropriateness for inclusion on this intervention. Whilst other difficulties, such as behavioural problems and low mood may also be present, the programme specifically targets anxiety and this should be the primary presenting problem.
This intervention involves six sessions for 6 parents and 2 key school staff members. Parents and staff are required to read relevant chapters from an accompanying book titled, ‘Overcoming Your Child’s Fears and Worries’ (Cathy Creswell & Lucy Willetts, 2007).
The aim of the programme is for parents to become anxiety management experts who can continue to use the strategies they have learned to help their child after the sessions have finished. It also means that children do not have to miss school or other activities to attend sessions. As such, the philosophy of the programme is non-blaming and one that highlights positive skills and responses of the parent, in order to build their confidence and empower them to support their child.
Expectations for parents or caregivers:
- attending all 6 x 1.5 hour face-to-face group sessions
- purchasing the book ‘Overcoming Your Child’s Fears and Worries’ (Creswell and Willetts, 2007) for sale at online bookstores or gaining a copy from a library
- reading the relevant sections of the book alongside attending all sessions
- completing all homework tasks each week in between sessions
- parents should not be engaging in other therapeutic treatments for their child during the course of the programme
- attending a preliminary and follow up session to complete assessments and evaluations
Key area of need
All types of anxiety for children and young people with or without a diagnosis of anxiety or ASC or ADHD.
Age group
Suitable for all ages.
This intervention is conducted solely with parents (carers or guardians) –children do not attend. In order for strategies to be implemented consistently, it is imperative that one parent commits to attending all the group sessions and that this parent is motivated and in a position to make relevant changes in their child’s life. If the other parent is able to join some of the session (with the agreement of the other group members) that will be very helpful and communication of what is covered in sessions should always be encouraged.
This programme can be delivered individually to parents also.
Useful links to research
Thirlwall, K., Cooper, P., Karalus, J., Voysey, M., Willetts, L. & Creswell, C. (2013) Treatment of child anxiety disorders via guided parent-delivered cognitive-behavioural therapy: randomised controlled trial. The British Journal of Psychiatry, 203 (6) 436-444).
Where can I access information about this?
Educational Psychology Service – https://www.devon.gov.uk/support-schools-settings/send/educational-psychology/educational-psychology-service/
Evidence base
Evidence includes CAMHS and Educational Psychology Service evaluations of completed programmes with parents or caregivers.
A number of NHS CAMHS services now use the Overcoming Programme as their first line treatment for childhood anxiety disorders. Recent research trials suggest that the Overcoming Programme with parents is at least as effective, if not more effective, than many comprehensive CBT interventions delivered one to one with a child.
The Devon Educational Psychology Service has conducted a number of groups and evaluated the effectiveness of the group in mainstream and specialist settings, with and without members of staff as well as parents. Evaluations have been positive and parents and staff have reported a variety of improved outcomes and reduced anxiety experienced by the children and young people.
Limitations to research evidence
Research is in this area is in its infancy and research into the group delivery of this programme is yet to be peer reviewed.
Research references
Thirlwall, K., Cooper, P., Karalus, J., Voysey, M., Willetts, L. & Creswell, C. (2013) Treatment of child anxiety disorders via guided parent-delivered cognitive-behavioural therapy: randomised controlled trial. The British Journal of Psychiatry, 203 (6) 436-444).