Standard Operating Procedure (SOP) for Older Persons Care Homes Version 1 February 2026
1. Purpose, Scope, Legal Framework & Principles
1.1 Purpose of the SOP
- To support effective and equitable implementation of Adult Social Care, Residential & Nursing Care Home 2025 Pre-placement Agreement (2025 PPA)
- Replace Resource Allocation System (RAS) /Personalised Fee Model with the Older Persons Fee Model
- Provide clarity, consistency and high quality in assessment and placement processes
- Ensure practice aligns with The Care Act 2014, as amended by The Health and Social Care Act 2022; Choice of Accommodation Regulations 2014; current Statutory Guidance and Devon County Council (DCC) policies
1.2 Scope
- For all people involved in assessment, arranging, and monitoring older persons care home placements in residential and nursing homes.
- Applies to all Devon-based providers signing the 2025 PPA.
1.3. Out of Scope
- Hospital Discharge arrangements until the Care Act Assessment has been completed.
- Out of County placements
1.4 Legal & Policy Framework
- Care Act 2014 as amended by the Health and Care Act 2022 (assessment, eligibility, choice, personal budgets, reviews); Mental Capacity Act 2005; Human Rights Act 1998, and other relevant legislation
- DCC “Choice in Care Policy”
- Top-Up Policy
- Deferred Payment Agreement Policy
- Charging and Fair & Affordable Care Policies
1.5 Principles
- Effective Partnership working and robust collaboration
- Strengths-based approach (“Three Conversations”)
- Fair & Affordable, Promoting Independence, Choice and high quality
- Accuracy, transparency, and consistency
2. Person’s Care Journey & Touchpoints
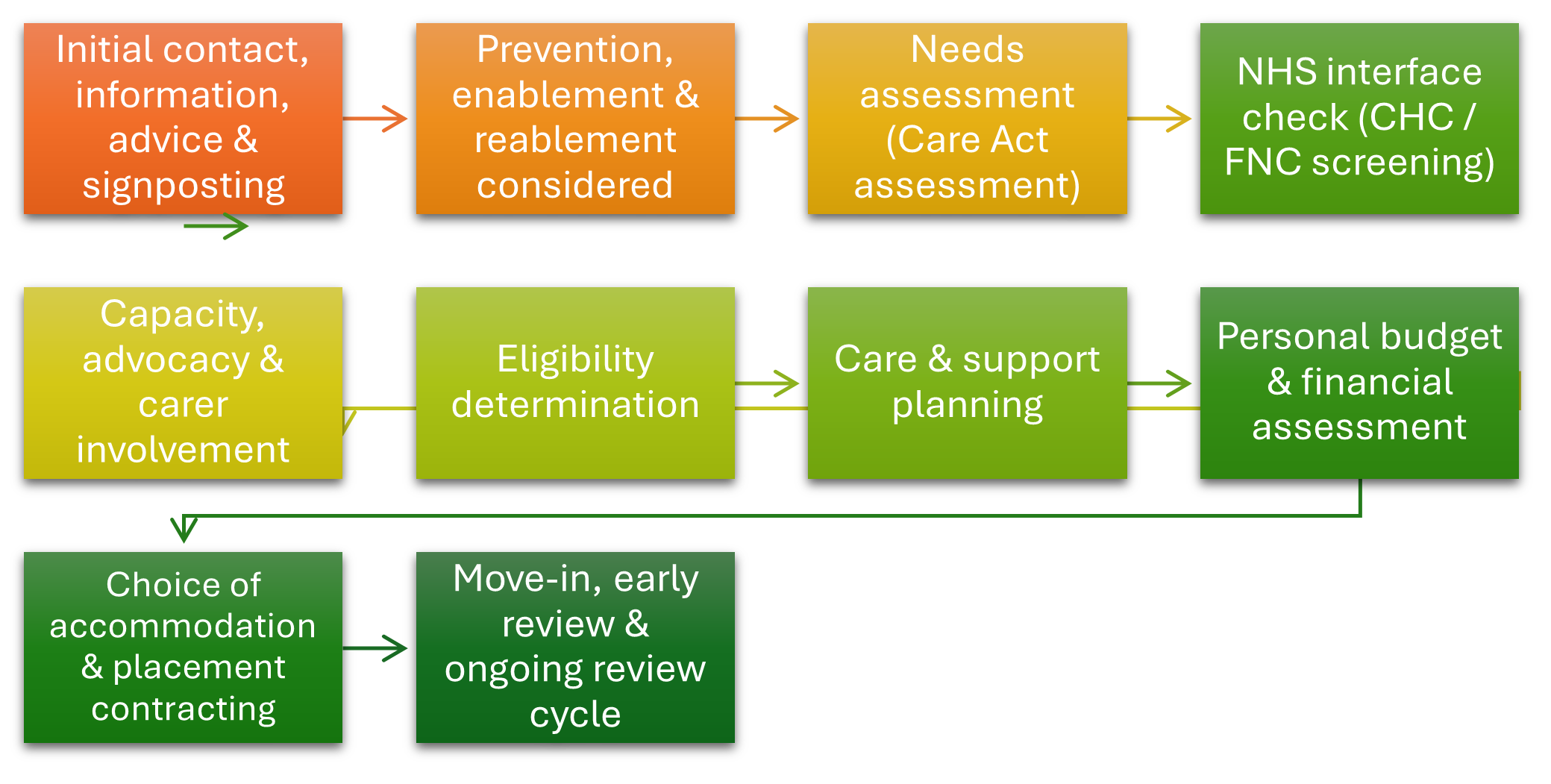
2.1 Initial Contact, Screening & Information Duty
- Local Authority (LA) offers accurate information, services and advice through accessible resource including website
- Adult Social Care Teams support prevention and reablement
- Care home placement consideration may arrive via community, hospital discharge, or capital depletion; and relevant information from a person’s care journey, must be brought into the assessment, including information from practitioners, providers and health teams.
- Practitioners must ensure professional, supportive and timely communication with people, families, and providers
2.2 Care Act Assessment
- Assessment must determine needs and eligibility, fairly and reasonably
- Use information from the person and family including their goals
- Use information from current providers where available
- Information from multi-disciplinary teams’ support understanding of health needs
- Ensure sufficient, robust and accurate evidence
- Discuss with the person whether the Care Act Assessment may be shared with the provider and if yes, whether there is anything within it they do not wish to share.
2.3 Planning Support to meet eligible needs
- Consider alternatives to care home placement
- Consider provisional indication of whether the person will rely on public funding or be using their own funds and trigger financial assessment where required.
2.4 Determining Needs & Applying Service Descriptors
- Use Service Descriptor 11 categories for both residential and nursing placements.
- Effectively consider nursing needs (including consultation with community nursing and Providers)
- Consider Continuing Health Care (CHC) where relevant, triggered via checklist; NHS assessment will determine CHC/Funded Nursing Care (FNC)
- Practice Quality Forum (PQF) validates residential/nursing Service Descriptor Level (Residential or Nursing, or bespoke care arrangements*) outcome and the Devon Integrated Adult Social Care (IASC) personal budget level.
- Bespoke Care arrangements* are considered and agreed by the Enhanced Authorisation Process (EAP) (further details in section 2.13).
2.5 Financial Assessment, Personal Budgets & Charging
- Trigger financial assessment when LA funding is required
- Consider additional financial pathways (1st and 3rd party Top Up’s) as detailed in section 3 below, providing information for the person and their family
- Ensure person/family understand financial commitments and the documentation is signed.
- Confirm placement details after funding confirmed
- Ensure person/family understand financial commitments
2.6 Choice of Accommodation
a) Must meet needs
b) Must not exceed the normal rate that the Local Authority would usually expect to pay (unless top-up arranged)
c) Must be available
d) Provider must have signed the Adult Social Care, Residential & Nursing Care Home Pre-placement Agreement
e) Additional choices, options and features may be available if funds are available to top up.
2.7 Brokerage & Market Engagement
Search radius steps:
- Search A: Preferred area + 5 miles (2 days)
- Search B: 15 miles (2 days)
- Search C: Countywide
Steps: - Arranging Support Team (AST) → market search
- AST → share offers at personal budget
- Practitioner → discuss with person/family
- Practitioner → confirm preferred option
- AST → confirm placement and start date
- AST → share Your Care and Support Plan (YCSP) within 48 hours.
- Ensure full case recording
2.8 Move-In Process
- Provider shall undertake an assessment of the person prior to final agreement of placement
- Introduction to the home/person
- Person/family supported to understand arrangements
- Providers receive Your Care and Support Plan (YCSP) and other essential documents are sent to providers within 2 days of the placement starting
- Confirm placement start, contract terms, costs
2.9 Initial Review (6–8 weeks)
- Light touch review with practitioner, provider, person and family
- Confirm suitability of placement
- Review Service Descriptor assessment if the persons needs have materially changed, requirement to take this back to PQF for sign off
2.10 Annual Reviews
- Annual assessment using 11 Service Descriptor category areas
- Essential person and family involvement
- Provider input also required
- Outcome of assessment discussed with provider (Manager/Senior Staff member)
- PQF oversight and authorisation
- Communicate outcome to provider and person
- Your Care & Support Plan is updated and shared with provider and person.
2.11 Escalation to seek resolution of disagreement.
- If the person or provider does not agree with assessment outcome, they can provide additional evidence to support against relevant Service Descriptor categories If agreement cannot be reached, Manager oversight is sought (DCC team manager to manager within the provider service)
- The final stage of escalation will be Community Service Manager level (DCC) to equivalent manager within the provider service.
- If agreement has not been reached at manager discussion DCC Older Persons Practice Lead may be asked to review the case if all parties agree that the Practice Lead decision is final.
2.12 Addressing short term escalation in needs
- Applies when significant increase in needs across multiple Service Descriptor categories.
- This section applies where the escalation in need is believed to be temporary
- Clear evidence of escalated needs and requirements.
- Health professional involvement mandatory
- Explore any Technology Enabled Care and Support (TECS) that may be appropriate (if any) before escalation
- Time-limited Targeted Support may be considered (if considered temporary)
- Agreement through PQF then Enhanced Authorisation Process (EAP) for approval
- Provider must keep adequate care notes including behaviour diaries where requested.
- For urgent escalations the Assistant Director (AD) for the Locality in which the Care Home Operates can agree time limited targeted support which will be reviewed as appropriate at the next available EAP.
- Where the change in need is understood to impact long term, a re-assessment under the service descriptor framework should be arranged (i.e. bringing forward the annual review).
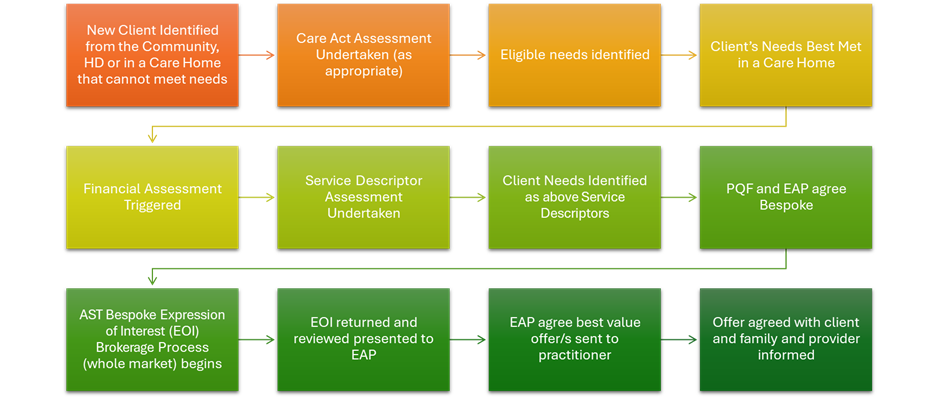
2.13 Bespoke Care Arrangements
- Applies when during the assessment process the persons needs are identified as exceeding the level of care outlined in the Service Descriptors (R3 and N5) in multiple areas.
- PQF → EAP approval
Bespoke Care Arrangements– New Clients
- AST & practitioner complete information form to invite Expression of Interest (EOI)
- Providers respond within 2 days – including costs for services offered on the pricing sheet.
- DCC Finance validate costings
- EAP authorises best value option
- Practitioner discusses with person/family and provider and finalise placement arrangements
Bespoke Care Arrangements – Existing Clients
- Care Manager completes Part A of the Long-Term Bespoke Review form and sends with Part B and the pricing template for the provider to complete
- Provider submits Part B and pricing template
- DCC Finance validate costings
- EAP review EOI and costs and agree or reject
- If rejected → return to EOI process indicating this is a repeat process
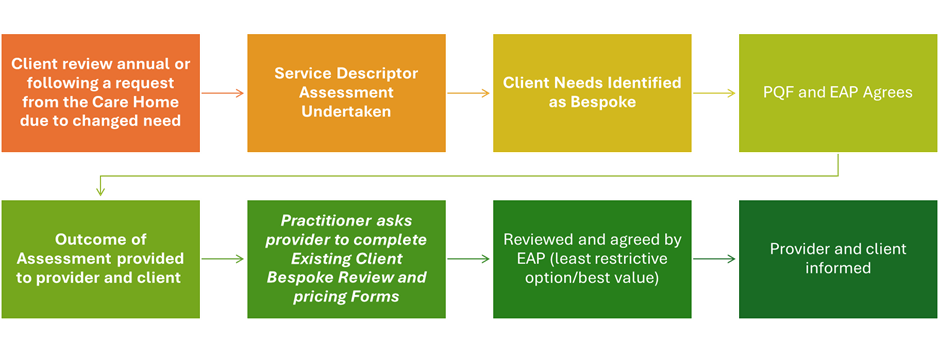
Bespoke Reviews
- 4-week review includes plans to step down support and costs as/if person settles
- Annual review process including provider input as detailed in section 2.10 above
3. Financial Pathways & Governance
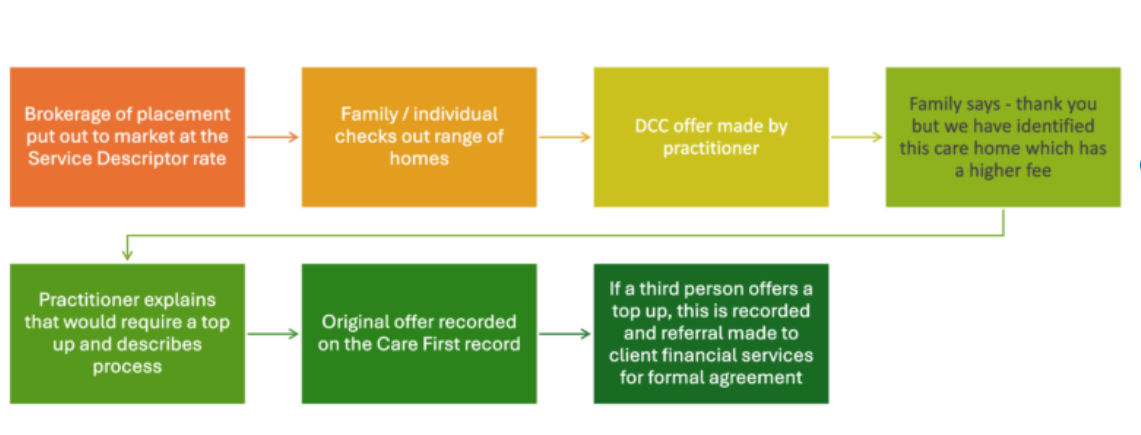
3.1 Third-Party Top-Ups
- Can be a funding contribution only where the following apply:
- there is a suitable option at the agreed local authority rate And
- where person chooses a placement at cost above the LA usual rate; And
- There is a third party willing and able to contribute the difference, for the foreseeable duration of the placement.
- Must be agreed in line with the DCC Top-Up Policy
- Written top-up agreement with the third party required
- Practitioner signposts person to guidance and Client Finance Services referral is made
- DCC (Practitioner and/or Client Financial Services) must ensure parties understand sustainability requirements of the agreement; including that the person may need to move if the top up cannot be sustained; and that the third party has given a realistic commitment to pay the top up for the foreseeable future.
3.2 First-Party Top-Ups
- Allowed only when:
- Deferred Payment Agreement is in place
- 12-week property disregard applies
- s117 applies (with specific arrangements)
3.3 Top Up policy and process
- All Top Ups must be agreed between DCC, the specified Care Home, the person/and or the third party. They are paid direct to DCC who then pays the Care Home the full amount.
- Refer to DCC Top Up Policy, see appendix 6.
3.4 Deferred Payment Agreements (DPA)
- Person may defer costs if they meet DPA eligibility
- Practitioner signposts person to guidance; financial assessment required
- Person may choose to fund top-ups
- Refer to DCC DPA Policy for full process
3.5 Personal Budget, Contract Price & Payment Mechanisms
- Personal Budget reflects assessed needs detailed in the Service Descriptor level and Care Act needs and requirements assessment outcome.
- Updated following reviews; the provider will support information gather/evidence
- Provider must be informed of Service Descriptor assessment level outcome (see formal escalation processes if provider does not agree with assessed level of need)
- Contract price (the Service Descriptor level outcome and Care Act needs and requirements) must be communicated to providers.
3.6 Additional Costs and Services
- A Care Home may offer additional services that go beyond the care and support needs identified in the persons Your Care and Support Plan. These might include
- Additional Therapies (e.g. Physio, exercise class)
- Recreational activities (e.g. social clubs, outings)
- Supplementary health services (e.g. dental, vision care)
- Hairdressing / dry cleaning
- These extras are not considered essential or core services under the care act and charges will be funded by the individual privately.
- Payments for these services should not be confused with Top Ups.
- Any charge or payment for additional services would be a direct transaction between the individual and the care home.
4. Local Authority ↔ Provider Interaction Points
4.1 Information Sharing
- Providers must update any changes in contact details through the online form on the PEN website
- Practitioners share YCSP and relevant assessments within 2 days of placement start.
- Providers cooperate with assessments and any moves are compliant with the legislation and policy framework.
- Providers complete Quarterly monitoring reports during the KPI pilot and following implementation from April 2027.
4.2 Operational Communication Routes
- AST contact for placement offers
- CDP contact for review requests
- Practitioners communicate assessment outcomes
- All cases to be managed by a named individual during any given assessment or review episode, with contact details of that LA assessor being shared with the provider. This would only be possible for the duration of any individual assessment or review episode as people do not remain on the caseload of any named individual in between these points of assessment.
4.3 Escalation & Dispute Resolution
- Provider → Team Manager
- Then → Community Services Manager / CDP Centre Manager
- If dispute about Service Descriptor level assessment outcome → consult Practice Lead (decision within 48 hours if parties agree to be bound)
4.4 Continuity of Care & Moves
- Providers should inform people/families from outset of a privately funded placement that a move may be required at point of capital depletion if the fee is above the LA rates (which can be found on the DCC website).
- Practitioner will discuss move with individual, family, and provider, exploring a third party top up if this facilitates choice
- Practitioner must assess risk before any proposed move – and seek authorisation for the person to remain where there would be a significantrisk to health/wellbeing.
5. Contractual Alignment, Quality Assurance & Market Oversight
5.1 Link to 2025 Pre-Placement Agreement
- Provider must have signed and returned the 2025 PPA to receive placements
- Contract governs payment, Service Descriptor framework, top-up rules
5.2 Monitoring & Review
- 6–8-week review
- Annual review
- Ad-hoc reviews
- Provider may request expedited review with evidence
- Providers complete quarterly KPI reports as requested.
5.3 Learning & Market Feedback Loops
- Provider concerns fed through escalation routes – see above
- Practitioner and provider feedback informs SOP improvement
- Information Resource Group (IRG) as an ongoing oversight and development forum with Providers to assist with good collaborative practice and implementation/review of this SOP.
- To identify and work together on process/system areas for improvement as appropriate.
6. Governance, Review & Version Management
6.1 SOP Ownership
- Senior Responsible Officer: Head of Quality, Performance & Re-design
- IRG supports development
6.2 Review Cycle
- Version controlled
- Review date to be set six months after launch and annually thereafter
- Amendments to be recorded formally
7. Appendices
- Contact details
- The Three Conversations model
- PQF and EAP Terms of Reference
- Templates (Bespoke forms, Top-Up Agreement to follow)
- Glossary
- List of policies:
Appendices
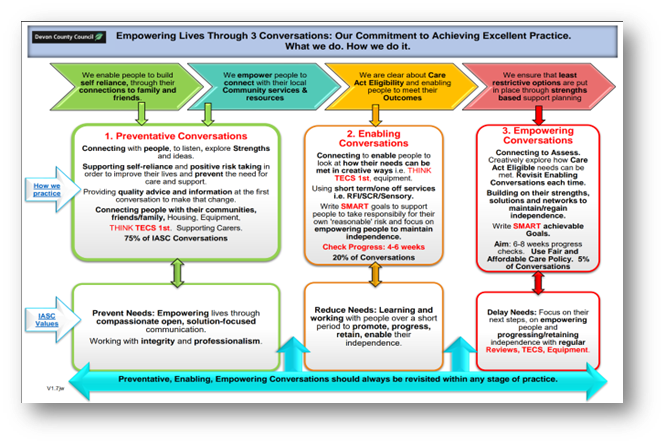
Appendix 1 – The Three Conversations model
The Three Conversations model is a strength-based framework for social workers to have deeper, more person-centred dialogues with individuals needing support, focusing on what matters to them rather than just assessing deficits. This approach aims to build relationships, use community assets, and provide more effective, less resource-intensive support. It involves three distinct stages:
Prevent: Having great proactive conversations, sign posting, advising, guiding, and supporting people to think differently.
Enable: Using short term intervention or enabling services, TECS, Equipment etc to change someone’s life around, supporting independence to regain or gain new independence.
Empower: within Care Act eligible care and support needs – what does this look like for someone? We include the above conversations, and ideas within reviews, for example. We might pause existing care and try something new. We look at what is happening for that person now and see if their needs can be met by TECS, new equipment, Apps, or other ideas. We then check back and review.
The picture below shows how DCC practitioners apply this model, and how it links to our core values.
Appendix 2 – Practice Quality Forum and Enhanced Authorisation Process: Terms of Reference
Purpose
Practice Quality Forums (PQFs) are collaborative spaces to apply the ‘Empowering Lives Through 3 Conversations’ approach; ensure compliance with the Care Act, and review care planning. They confirm that resources are used appropriately to meet outcomes and promote independence and wellbeing.
Principles
PQFs ensure quality, fairness, and creativity in care planning. They safeguard rights, promote independence, and provide a structured, supportive environment for decision-making.
Key Priorities
Apply strengths-based approaches protect rights; reduce dependency; and promote independence. Explore all options including community support and technology (Think TECS first). Encourage creativity and involve individuals and carers in planning.
Objectives
Drive best practice, improve decision-making, sign off care plans and budgets, ensure consistency across Devon, and provide governance for large or unique personal budgets.
Membership & Roles
Chaired by Community Services Manager (budget holder). Attendees include multidisciplinary teams (DCC, NHS). Team Managers and practitioners present cases; Practice Leads support complex decisions.
Enhanced Authorisation Process
The Enhanced Authorisation Process, chaired by Deputy Director of Head of Service, applies in situations where there is a value in bringing senior managers and commissioners to provide expertise to support the decision-making. At present, this additional focus is given to situations where Bespoke pricing; targeted support; or additional payments may apply.
Appendix 3 – Glossary of terms
| Title | Full Phrase |
| ASC | Adult Social Care |
| DPA | Direct Payment Agreement |
| CQC | Care Quality Commission |
| OT | Occupational Therapy |
| IASC | Integrated Adult Social Care |
| LMEW | Leading & Managing Effective Workflow |
| DoLS | Deprivation of Liberty Safeguards |
| LPA | Lasting Power of Attorney |
| MCA | Mental Capacity Act |
| JACS | Joint Adult & Childrens System |
| DPA | Deferred Payment Agreement |
| AMHP | Approved Mental Health Professional |
| ICB | Integrated Care Board |
| MDT | Multi-Disciplinary Team |
| TEC | Technology Enabled Care |
| FOI | Freedom of Information |
| CHC | Continuing Health Care |
| PB | Personal Budget |
| SAS | Seaton, Axminster & Sidmouth |
| TC | Tiverton & Cullompton |
| HOSM | Honiton & Ottery St Mary |
| WEB | Woodbury, Exmouth & Budleigh Salterton |
| FNC | Funded Nursing Care |
| HDT | Hospital Discharge Team |
| STS | Short Term Support |
| KPI | Key Performance Indicators |
| LD | Learning Disability |
| P1 | Pathway One Discharge |
| P2 | Pathway Two Discharge |
| P3 | Pathway Three Discharge |
| D2A | Discharge to Assess |
| CwA | Care with Accommodation |
| O65 | Over 65 |
| U65 | Under 65 |
| MS | Microsoft |
| AI | Artificial Intelligence |
| AST | Arranging Support Team |
| CSO | Commissioning Support Officer |
| CO | Commissioning Officer |
| CDO | Commissioning Development Officer |
| PQF | Practice Quality Forum |
| DLG | Directorate Leadership Group |
| CSEG | Care Services Escalation Group |
| CHSC | Community Health and Social Care |
| BCF | Better Care Fund |
| SOP | Standard Operating Procedure |
| PID | Project Initiation Document |
| BRO | Business Relations Officer |
| MPS | Market Position Statement |
| CFP | Competitive Flexible Procedure |
| DPS | Dynamic Purchasing System |
| TSA | TEC Services Association |
| FPS | Flexible Purchasing System |
| ECH | Extra Care Housing |
| DPT | Devon Partnership Trust |
| TOR | Terms of Reference |
| UCR | Urgent Community Response |
| DLG | Directorate Leadership Group |
| SLT | Senior Leadership Team |
| ROD | Record of Decision |
| POP | Practice & Operational Process |