Contents
Autism
Services for needs including autism, speech language and communication or social, emotional, and mental health needs are delivered at the right time.
Local Needs
Autism affects people in varying ways, with different people having very different strengths and weaknesses. It is therefore especially important that support is personalised and takes into account the individual’s strengths, needs, views and circumstances.
Based on population prevalence measures, an estimated 7,987 5-24 year olds in Devon have a neurodevelopmental disorder, of which 1840 have autism and 3812 have a learning disability[18]. The prevalence of child disability – including neurodevelopmental disorders – increases as socio-economic status decreases. Intellectual and developmental disabilities are strongly associated with socio-economic disadvantage, whereas the association is weaker for physical disabilities. Parents and children from disadvantaged households may be more exposed to risk factors such as inadequate nutrition, environmental pollutants, unsafe housing, tobacco smoke and infections. These factors may interact with other risk factors which may increase the risk of being born with or developing a disability, as well as negatively affecting their condition[19].
While only 6% of SEN support relate to autism, it is the primary need of around 27% of EHCPs in Devon. This suggests a shortcoming in the early support offered to children and young people with identified autism needs to prevent escalation of needs. The number of children and young people in Devon with diagnosed autism exceeds national prevalence figures. For example, the number of Education Health and Care Plan’s (EHCP’s) with autism as a primary need totalled 1935 as of January 2021 – having more than doubled since 2018. Of those children and young people undergoing an autism assessment, currently 86% receive a diagnosis; this has remained stable over a number of years but is higher than other reported areas who report 75-80% and studies who again report lower rates[20]. This recent and rapid increase in autism assessments – with the rate of diagnosis remaining stable – suggests that early needs are not being met effectively. This is leading to an escalation of the education, health and care support required by these children and families, where a diagnosis is the key to accessing the help that they need. This plan sets out our steps to address this.
During 2020, alongside Young Devon and Parent Carer Forum Devon, we engaged with over 300 children and young people and families who are currently on the autism assessment waiting list through direct conversations as well as a survey. They told us that they experience long periods of time on the waiting list, often without regular and appropriate communication, information, or support. Families told us they want improved communication and information about the process, the wait times and what happens during and after an assessment. They also made clear that it would be important to have signposting services, including an online resource, from which they could access more advice, support, and guidance. What they told us is directly informing our steps to improve services for children and young people with autism.
[18] Devon’s Joint Strategic Needs Assessment for Children and Young People with Special Educational needs and Disabilities (SEND) 2017, published by Public Health Devon, page 41
[19] Devon JSNA for children and young people with SEND, page 56-57
[20] https://www.healthyork.org/media/62035/autism-needs-assessment-2016.pdf) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6513463/
Where we are now
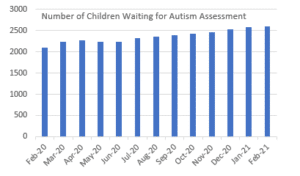
The Autism Assessment Service is commissioned by the CCG and is provided by Children and Family Health Devon (CFHD). Currently, in Devon, there continue to be prolonged delays in the autism assessment service. As a Partnership, we know this is not acceptable because of the negative impact creates for children and their families. 2,844 (March 2021) children and young people are currently on the assessment waitlist, up 44% from 1800 when the contract transferred to CFHD.
Some families are waiting up to 18 months for an assessment and the average length of time that children are waiting has also increased by 30% between February 2020 and February 2021 (the current median wait-time is 82 weeks).
The prolonged delays waiting for an autism assessment result from service provision being unable to keep pace with demand, with insufficient clinical capacity to clear the backlog. Demand has increased by 75% in the three years to 2019-20, while, during COVID, the referral rate only dropped by 25%. Changes to senior leadership, workforce instability and the challenges of the pandemic have also exacerbated the delays.
We are committed to working together to change this. The needs of all the children waiting have been reviewed and additional support has been put in place while they are waiting. This includes regular contact with families and access to other services who can offer support such as speech and language teams and CAMHS. All families, on the waitlist, have now been communicated with on up-to-date wait times and signposting to online resources and workshops. CFHD are building this into the service and embedding the learning.
In addition, to support young children with neurodevelopmental needs, Children’s Centres have developed specialist capacity through the expansion of the multi-agency Increasing Access to Psychological Therapies (IAPT) programme. The expansion of the programme seeks to identify and support neurodevelopmental needs early on, helping children and families access the help they need.
We have also undertaken training and awareness raising to schools and settings throughout 2018/19 called the Devon Enhanced Language Programme and the Devon Enhanced Autism Programme. Education and Inclusion services continue to support schools to adopt strategies in line with the graduated response which meet the needs of children early in their education setting. Specialist support is also available from the Communication and Interaction team and Behaviour Support teams currently provided by Babcock. Further details of our progress in improving services for children with autism can be found in the latest Written Statement of Action (WSoA) Progress update.
We are committed to delivering a continuum of support for children as they grow and develop. Including tailored support for complex neurodevelopmental needs in children that may trigger periods of crisis or significant needs which disrupts participation in everyday life.
DCC also commissions individual support for families following assessment of need. In partnership with parents and carers, sometimes the chosen offer of support and intervention is delivered via the use of the BisNET service provided by CEDA if it is felt to best meet need. This service offers; Training services for parents and carers, relationship Development Intervention (RDI®) consultation, Family Therapy service, Community Support.
What we will do
Through the SEND Transformation, children and young people with neurodevelopmental needs will be supported through a system-wide, multi-disciplinary redesign. We will set this out in our Autism Strategy. Parents and carers have told us that the waiting times for assessment and diagnosis are too long and have a significant impact on families. The lack of a clear offer of support early when the needs of children first present is also an area for development. This feedback, combined with the performance and the needs data above, have led us to setting the priorities below.
Getting Advice
- Ensure there is easier access to information, support, advice, and training for families through an improved online offer which has resources and online workshops
- Extend access to telephone support for families and practitioners provided by specialist autism practitioners
Getting Help
- Develop and embed autism expertise within the Early help offer to families
- Roll-out the joint funded pilot health navigator/connector role during 2021, embedding the roles within the Early Help offer and coordinate pre assessment support
- Provide training to develop the skills and confidence of the multi-agency workforce to meet individuals’ needs as an alternative to referring for a diagnostic assessment as well as being able to contribute to the assessment process.
- The Youth Service and our careers advice and support service, CSW Group (formerly Careers South West), will ensure the support for young people with autism is comprehensive and effective, including by improving the skill, knowledge, and competence of staff in supporting children and young people with neurodevelopmental disorders. For the youth service, this is being actioned through Space’s staff development.
- Expand and evaluate the national Key Worker Pilot. Key Worker pilots have now been established (Devon is one of the 13 locations) in response to the NHS Long Term Plan commitment, that by 2023/24, children and young people with a Learning Disability, autism or both will have a designated Key Worker.
- Revise the criteria for assessment and identifying the core support that is required prior to referral for diagnostic assessment. This will improve the pathway of support, from the date of referral and the advice that is given to parents and carers as well as improve the timeliness of assessments
- Improve support for families with children with autism or similar needs. This will be through a health led Community Intervention offer an evidence-based programmes such as Early Bird[21] and ASCEND[22].
- Review and expand the family support offer for children over the age of 8 with neurodevelopmental needs. Family Intervention Team and some small VCSE providers. The offer will be reviewed and increased by Summer 2021.
Getting More Help
- Resolve the number of children waiting for an assessment and reduce the length of time that children and young people are waiting for a diagnostic assessment by November 2021
- Pilot a new Nurse for Care Leavers role in 2021 and ensure professionals know where and how care leavers can access additional support where they have a diagnosis or a suspected diagnosis of a neurodevelopmental need. As corporate parents, we will ensure children in care and care leavers are supported as a priority group.
- Using the resources available through the NHS Long Term Plan for Learning Disability and Autism develop the Learning Disability Service with a multidisciplinary team offer including SALT and OT capacity to respond to the needs of children with autism and children with a mild to moderate learning disability. This will be connected to both a complimentary early help offer to meet need early or offer step down support but also take an assertive outreach approach to provide support where families need more help. This will also address the current gap for family support for children with Pathological Demand Avoidance.
- The review and re-commissioning of Devon’s Short Breaks will deliver an offer which reflects the neurodevelopmental needs of children and young people, by Spring 2022.
How we will know we are making a difference
Outcomes for children and young people
- Outcomes at Early Years Foundation Stage (EYFS) for children with autism have improved
- Pupils with autism as a primary need of an EHCP or SEN Support are achieving better educational outcomes
- Fewer pupils with autism are being excluded or inappropriately electively home-educated
- Early tailored support for children with autism to prevent routes into offending
- Children will be prevented from experiencing crisis or family breakdown by receiving support at the right time and early.
- Children without a diagnosis but in need of tailored specialist support receive this at the right time.
Outcomes for services
- The assessments and diagnoses are undertaken within the 18 week referral to treatment time
- Children and families have easy and early access to the support they need
- We are supporting more children with neurodevelopmental needs at a younger age and can demonstrate an expanded offer of advice, guidance, and support to children who have autism or autism traits
[21] Family support (autism.org.uk)
[22] About Ascend Autism | Behaviour Analysis Company Westchester NY
Speech language and communication
Local needs
It is widely accepted that over 10% of all children and young people have some form of speech, language, or communication need (SLCN) that persists and impairs their social and/or educational functioning. 2.5% of children have a language disorder associated with another biomedical condition, such as autism, learning disabilities, sensory-neural hearing loss, cerebral palsy, or Down syndrome. While around 7.5% of children have a language disorder that is not associated with another condition. This is known as Developmental Language Disorder. In addition, it is estimated, that in areas of high social deprivation across the UK, between 40% and 56% of children start school with communication difficulties.
In Devon, it is estimated that there are 33,339 children and young people with speech, communication, and language needs (SLCN), aged 0-24yrs[23]. It is important to note that whilst these figures are not indicative of all children and young people needing direct speech and language therapy, they are indicative of the demands placed on the speech and language therapy (SLT) service to support whole system change.
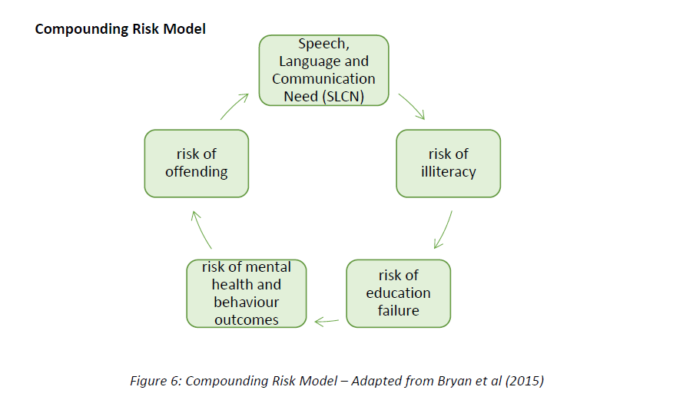
SLCN are a significant risk factor for poor educational attainment, employability, offending and Social, Emotional, Mental Health (SEMH). Research has shown that 81% of children with emotional and behavioural disorders have significant unidentified language deficits[1]. The presentation of communication difficulties is common in children and young people accessing mental health services. SLCN and SEMH are also disproportionately found in populations of children and young people in care or known to Youth Offending services. The diagram shows the compounding risks and vulnerabilities that stem from SLCN.[25]
The needs analysis undertaken in 2019, supported by Marie Gascoigne (Better Communication CIC) and the Balanced System® online mapping tools found that the ratio of speech and language therapists to local SLCN as 1.54 WTE per 1000 population of predicted children with SLCN. Which is below a nationally recognised ratio of 1.9 and 2.2 Whole Time Equivalent SLT per 1000 as good local practice. It also found a shortfall in the sufficient levels of professional expertise, skills, and knowledge in meeting SEMH needs at all levels, as well as a need to strengthen the advice and initial help and support we give children and their families.
In February 2021, there were 2,631 children and young people on the SLT wait-list. This is a 40% increase on the wait-list numbers in February 2020. This is in part an impact from COVID-19 and the standing down of services in during the first national lockdown. As a result of increasing pressures on services, more than half of these children and young people are waiting for longer than the 18-week threshold, while the numbers waiting over 52 weeks for treatment has substantially increased to a total of 382 – almost 15% of all those waiting.
[23] This is based on a composite index based on the prevalence of existing diagnosed disorders which affect speech, language, and communication, as well as an assessment of levels of disadvantage which is likely to lead to poor development of early language and communication skills.
[24] Hollo A, Wehby JH, Oliver RM. Unidentified Language Deficits in Children with Emotional and Behavioural Disorders: A Meta-Analysis. Exceptional Children 2014; 80(2): 169-186. http://journals.sagepub.com/doi/abs/10.1177/001440291408000203
[25] 2015. Bryan, K, Garvani, G, Gregory, J and Kilner, K. Language difficulties and criminal justice: the need for earlier identification. International Journal of language and Communication Disorders, 50. 763-775. Doi: 10.1111/1460-6984.12183.
Where we are now
Communication is everyone’s business. Health, education and social care, alike, all have a role to play in improving outcomes for children and young people with SLCN. However, feedback shows that often this support can appear fragmented to those accessing it. Within the Improving Access to Communication Services and Support (IACSS) programme, commissioners, service providers and parents and carers work together and focus on transformation to ensure there is an integrated approach to supporting SLCN. In addition, there is a specific focus on children and young people with social emotional and mental health (SEMH) needs, the antenatal to 5 years of age cohort of children, as well as the use of Augmentative Alternative Communication (AAC).
The Improving Access to Communication Services and Support (IACSS) programme started in 2018 with the aim of addressing key areas of improvement and development with the support of national expertise and a national tool to analysis the needs of our local population. It covers the Torbay, Plymouth and Devon combined area and reports to SEND boards in each local authority area, with governance from local safeguarding Partnerships where necessary. The Programme’s key aims focus on improving outcomes for children and young people with SLCN through prevention and early help, including workforce capacity building, and a focus on ‘right support at the right time in the right place’.
What we will do
The analysis of local needs set out above and the feedback from parents and children on the impact from lack of early support have led to the priorities set out below:
- Monitor and assess the impact of COVID on the needs of children. Established recovery actions will be jointly funded and delivered.
- Address the waiting list and the increased demand for speech and language therapy by funding additional capacity, including for those children with EHCP and SLT needs, by September 2021.
- Children and Family Health Devon (CFHD) to bring in additional expertise to lead their service transformation and bring in a competency framework review to upskill staff. Subsequently, CFHD will offer training to the wider partnership workforce.
- Review and increase the partnership wide training offer so that the workforce has the skills to understand the connections between SLCN, mental health, Adverse Childhood Experiences (ACEs), trauma. Ensuring key messages regarding the links between SLCN and SEMH are explicit in all key training resources, policies, protocols, and procedures (e.g. the Graduated Response profiling tool)
- Develop and train a specialist response to meet SEMH needs within our population using SLT approaches[26].
- Address the gap in expertise and identification of Developmental Language Disorder.
[26] This will include 7 SLTs in CFHD, 1 in YOT and 2 in the Edge of Care service (Bridges).
Alternative Augmentative Communication (AAC)
Arrangements are in place that jointly commission a specialist AAC service provided by Vranch House that supports children and young people with their AAC needs, this service sits between the broader SLT offer provided by CFHD and a specialist service commissioned by NHSE AAC West of England Specialist Team (AAC WEST). During 2019-2020, the IACSS Programme completed a review of Alternative Augmentative Communication (AAC) practice and provision across the Devon, Plymouth and Torbay. An improvement plan has been developed and progress is reported to the SEND Board.
To achieve our ambitions, we will maximise joint commissioning arrangements to:
- Ensure the local training offer to stakeholders is clear and accessible and considers the areas highlighted in survey results & addresses gaps
- Promote more effectively local and national resources to improve accessibility
- Ensure the AAC offer is accessible with clear eligibility and referral processes and systems are in place to ensure there is a continuum of appropriate support available.
Antenatal-5 years
Early language development and communication skills are recognised as primary indicators of child wellbeing (Language as a child wellbeing indicator EIF). The ability to communicate is the most fundamental life skill for children; it is essential to learn, develop friendships and improve future life chances. Parents, caregivers, and those closest to the child, have a primary role in supporting speech, language and communication development, are best placed to provide language rich environments for their children and are the key partners in the early identification of needs. Consequently, the antenatal-5 years workstream are working collaboratively to strengthen the universal offer for children and their families.
We will:
- Develop the skills, knowledge and confidence of the universal workforce so that ‘every contact counts’, know when to be concerned and understand what signs indicate a child may have difficulties in speech, language, and communication, have simple strategies available to support development, know who to talk to about concerns and where to get advice
- Strengthen access to evidenced-based information and resources regarding typical development and how adults can support a child’s speech, language, and communication development. Develop access to specialist staff for advice and guidance.
- Implement the new Public Health England Guidance and Tools to support early identification and intervention (PHE Best start in speech, language and communication)
How we will know we are making a difference
Outcomes for children and young people
- Increasing numbers of children reach expected levels in Communication, Language and Literacy at Early Years Foundation Stage (EYFS)
- Children and young people with SLCN and/or SEMH needs are achieving better outcomes at school – measured through the academic outcomes of pupils with EHCPs (with SLCN or SEMH as primary need or secondary need) at the end of each Key Stage. Inequalities between different groups of children and young people have reduced, including children and young people in care who have SEMH and/or SLCN.
- A reduction in the proportion of children with SLCN who receive one or more fixed term exclusions from school
- A reduction in the number of children and young people, known to YOS, whose SLCN needs had not been previously identified
- Children, young people, parents, carers and families tell us, through surveys, interviews and focus groups, that they able to access the support they need more easily, at the right time, that they have increased trust and confidence in services
Outcomes for services
- Children who are supported in specialist SEMH provision routinely screened for SLCN needs to ensure SLCN needs are met
- An overall reduction in the number of children waiting for an assessment. Currently there are 2864 children who are waiting of which 45% are waiting under 18 weeks and 13% are waiting more than 52 weeks. An increase in the proportion receiving treatment within the 18-week target.
- Access to advice, guidance and support is expanded and accessed by an increased number of families
- Increasing evidence of the use of a graduated response prior to referral to specialist services
Annual Health Checks
Annual Health Checks (AHCs) play an important role in identifying learning disability needs as early as possible. The NHS Long Term Plan: Learning disability and autism sets out the ambition to increase the uptake of AHCs to 67% by 2020/21 and to achieve 75% by 2023/24 among people with learning disabilities, from age of 14 to 18. The latest figures, for Spring 2020/21, show that 8% of 14-18 year olds, who are on a primary care learning disability register, have had an AHC. We are clear that this must improve. We have increased the use of local, up-to-date information to reduce the reliance on national data, which may be delayed. Commissioners are working with data and primary care teams to be able to interrogate data systems and identify how many young people, above 14 years of age, are on GP practices’ learning disability register and are receiving their AHCs.
What we will do
A grant from NHSE has been used to support the Devon Parent Carer Forum, to gather the views, and experiences of parent carers of children and young people with learning disabilities as well as young people themselves about annual health checks and whether they are well-known, well-attended and deemed to be useful. This started in March 2021 and will continue through to June 2021, informing the plan to increase awareness, knowledge and take up of the annual health checks.
Funded by the Burdett Trust, during 2021, a 12-month a pilot project is being led by nursing staff (primarily LD trained) to work with and provide direct support and advice to schools, primary care, and school nurses. Yung people will be supported to proactively write to their GP explaining a bit about themselves and asking to be put on the LD register, if not already, and invited to their AHC. The pilot also aims to improve the identification of young people with learning disabilities among schools, primary care, and school nurses through use of a newly-developed Learning Disability Toolkit.
How we will know we are making a difference
- There is an increased uptake of AHCs by young people on the Primary Care LD register aged 14 years in line with NHS Long Term Plan targets
- Achieve 100% of Primary care settings identifying as an LD champion by end of 2021
- Support a clear transition for children and young people with learning disabilities into their adult lives by promoting and supporting their ongoing health needs through Adult Learning Disability Primary Care Liaison Nurses.
Social emotional and mental health
We want all children and young people, right across Devon, to be living healthier and happier lives, with better mental health and overall wellbeing. This involves supporting families and schools to be settings which foster healthy psychological development in childhood and adolescence and delivering services that are effective, equitable and accessible, which lead to better outcomes and experiences for those who need them. Our ambitions for children and young people’s mental health services align with the aims of the Integrated Care System, national NHS Long Term Plan, principles of the THRIVE framework and the Community Mental Health Services Framework for Adults and Older Adults.
Local needs
The pandemic has had a significant impact on children and young people’s mental health and emotional wellbeing. The incidence of probable mental health issues among children, nationally, rose from 10.8% in 2017, to 16% in July 2020, and these children and young people were more than twice as likely to live in households that were falling behind with their bills as a result of the financial pressures of the pandemic[27].
For children and young people with SEND, even before the pandemic, mental health outcomes were generally much worse than the wider population. Children with learning disabilities were more than four times more likely to develop a mental health condition than those without, meaning 1 in 7 of all children and young people with mental health difficulties in the UK also have a learning disability[28].
Applying national estimates of the prevalence of mental health issues among children and young people with SEND to Devon’s population of children with learning disabilities suggests that there are almost a thousand children aged 0-19 who have some degree of learning disability accompanied by a psychiatric disorder[29]. Emerging evidence from the last 12 months suggests that COVID-19 will further worsen mental health outcomes for children and young people with SEND. In a national survey of parent carers of children with SEND, 70-80% reported a decline in mental health for their children and 64% said the lockdown was having a negative impact on their child’s condition[30].
Kooth, our online mental health and wellbeing services, for children and young people 11 to 25, saw a significant increase in use between 1 March and 28 September 2020 with 413 unique users logged in, up from 331 in the same period in 2019. Anxiety/stress was by far the most common presenting issue for young people in Devon – 46.7% highlighted it as an issue for them, up from 33% in 2019. Body image, weight issues and eating difficulties all saw significant increases on 2019 levels, rising from only 38 young people reporting those issues, to 91 (and almost doubling as a proportion of all users between 2019 and 2020). Reporting of self-harm or suicidal thoughts rose from 102 to 163 young people, reaching almost 40% of all users.
At the beginning of national lockdown restrictions and the closure of schools for the majority of pupils, CAMHS referrals dropped by over half between March and April. However, there was an increase in the presentations of young people with additional and complex vulnerabilities. Referrals began to increase from September, with the highest number of 2020 coming in October which was 15% above the start of the year. The proportion of referrals accepted has remained steady between 65-70% throughout the year. With those not accepted offered signposted to Early Help 4 Mental Health and Kooth provision.
[27] Child mental health in England before and during the COVID-19 lockdown, published January 2021 by the Lancet Psychiatry
[28] Overshadowed: the mental health needs of children and young people with learning disabilities, published June 2019 by Children and Young People’s Mental health Coalition
Where we are now
NHS Long Term Plan and THRIVE
The delivery of the national NHS Long Term Plan in Devon is delivered through the Integrated Care System (ICS). The Long-Term Plan promises to increase investment in mental health services nationwide and improve mental health outcomes across the population as a result. Critically, there is a commitment in the Long Term Plan that investment in children’s mental health grows at a faster pace than investment in adult mental health. At a local level, the ICS builds the improvement of community mental health services in Devon around the principles of the THRIVE framework. A key element of the framework is to expand the prevention and early intervention of mental health needs through effective, collaborative multi-agency working to ‘make every contact count’ with children and young people. The framework recognises the role that all partners (including the voluntary and community sector) play in supporting the mental health and emotional wellbeing in every interaction they have with children and young people. Any intervention, in response to identified need, will be personalised, holistic, and strengths based. Inherent in the THRIVE framework is the understanding that supporting children and young people’s mental health needs has important cumulative benefits for other aspects of their lives. As such, we will maximise the mutual cumulative benefits of supporting good emotional wellbeing and mental health among children and young people for all local services.
[29] Devon’s Joint Strategic Needs Assessment for Children and Young People with Special Educational needs and Disabilities (SEND) 2017, published by Public Health Devon, page 44
[30] Left in Lockdown survey, results published in June 2020 by the Council for Disabled Children
CAMHS
The CCG holds a contract for children’s community health and wellbeing services with CFHD. This includes local Child and Adolescent Mental Health Services (CAMHS). Extensive feedback gathered from children and young people across Devon had highlighted CAMHS as an area for improvement within commissioned children’s community health services. Following national transformation programme investment, access to CAMHS had significantly improved. In recent years, the specialist community CAMH service is Devon has met the national targets to increase access to services. As numbers of children and young people accessing the service has risen, wait times, currently at 13 weeks, have been largely maintained at or better than the national median for referral to treatment. There has been an expansion of early intervention for mild to moderate level difficulties with Community Wellbeing practitioners, Recruit to Train posts and 3 Mental Health in Schools Teams. Work focussed on helping young people to avoid admission to CAMHS inpatient care has resulted in low numbers of admissions.
Early Help 4 Mental Health
Early Help 4 Mental Health (EH4MH) offers a framework of mental health support in Devon focused on prevention, early intervention, and multi-agency partnership working to develop links between schools and mental health services, as well as with wider health, primary care, social care, and voluntary and community sector partners. EH4MH is rooted in the THRIVE framework which provides help and support according to groupings based on individual needs. This begins with getting advice and help, then getting more help and risk support for high-level needs. EH4MH provides advice and help through two core elements: early intervention and schools-based support.
Early intervention for young people who are vulnerable, and have deteriorating mental health, includes community-based counselling and wellbeing conversations. While not specifically targeted at children and young people with SEND, eligibility for support is extended to those with SEND and/or care leavers up to the age of 25. The contract is currently delivered by Young Devon and funded by the CCG. In response to the pandemic impact on children and young people’s mental health, a 6-month extension to the core contract was agreed, with a further 6-month enhancement now in place to August 2021. Options will be explored to ensure the continuation of the contract for an additional 12 months, during which a longer-term procurement process can take place.
Kooth
As part of their mental health offer, CFHD sub-contracts an online emotional wellbeing and mental health support service for young people across Devon. Kooth offers a free, anonymous, and safe online mental wellbeing service, which is commissioned locally by CFHD. The service is for any young person aged 11-25 years old, and offers a range of advice, guidance, and support services. These include trained and qualified counsellors, discussion boards, live forums, and articles.
Mental Health in Schools Teams
Following the publication of the Green Paper: transforming children and young people’s mental health provision, NHS Devon was successful in securing funding for a Mental Health in Schools Team in wave Two (2019/20) and then a further team in Wave Three (2020/21). The Wave Two team have now completed their training and became operational during the current academic year. This team based in the Exeter area. The Wave Three team will be based in North Devon but are currently undergoing the training programme. A further application, in Waves Five and Six, for an additional team has been submitted and we are awaiting the outcome from NHS England and Improvement.
The Mental Health Support Teams will:
- Deliver evidence-based interventions for mild to moderate mental health issues
- Support the designated senior mental health lead in each education setting to introduce or develop their whole school or college approach
- Give timely advice to school and college staff, and liaise with external specialist services, to help children and young people to get the right support and stay in education.
16-25 mental health pathways for young adults
We know that one of the significant challenges facing our young people is the age-based transition between children and adult mental health services. We know from research and local practice that transitioning into adult services at 18 can be challenging for young people and we are currently working to improve the way that we support our young people with such transitions. In April 2019, NHS Devon awarded a contract for community health and wellbeing services for children and young people (including CAMHS), through which we signalled our intent to ensure pathways of support were available until the age of 25 years, in accordance with the 2014 SEND reforms. This intent has been aligned and reflected within our proposed model of delivery of support in relation to the Community Mental Health Framework. The Community Mental Health Framework model will ensure that any young adult, whether they are requesting help for the first time or are already known to services will receive integrated, holistic support.
Our model will ensure that any young adult, whether they are requesting help for the first time or are already known to services will receive integrated, holistic support personalised to their needs, developmental stage, life experiences and other vulnerabilities (e.g. being a care leaver, having a learning disability and/or neurodevelopmental differences). Building on the i-THRIVE model, we will ensure locality based early intervention and prevention support is aligned and integrated with our specialist mental health services. The roll out of this approach will begin during 2021/2022 and will be based around primary care networks at a locality level.
What we will do
In response to the NHS Long Term Plan priorities, the needs analysis data above and feedback from children, young people, parents and carers we have set the priorities below:
- By August 2021, we will undertake an analysis of the current mental health offer for all children and young people aged 0-25. This will be conducted considering current local need and demand on services. It will include an assessment of the impact of the pandemic on children and young people’s mental health and what that will mean for local services. While this will include all children and young people up to the age of 25, it will hold a specific focus on the needs of those with SEND and how services can better address those.
- From the assessment of current needs and demand, we will identify what level of support is needed. This will focus on strengthening the getting advice and getting help levels of offer. By September 2021 we will have an agreed system plan in place that will set out how we will address the identified needs and gaps and implement the necessary changes to mental health services.
- We will implement the Community Mental Health Framework plan and deliver priority services to young people 18-25 with SEND and who are Care Leavers. We will review the CAMHS to AMHS pathways and we will review the EH4MH, Kooth and Talkworks offer for 18-25-year olds.
- We will set out the priorities for delivery in line with the Long-Term Plan by June 2021 and identify resources over the next three years to meet the priorities.
How we will know we are making a difference
Outcomes for children and young people
- Children and young people with SEND are telling us that they can access the support they need to feel more resilient, and more hopeful for the future
- More children and young people with SEND have improved mental health and wellbeing & the gap between the mental health outcomes of children and young people with SEND and the wider population has narrowed – measured through CAMHS and EH4MH outcomes and proportion of children and young people accessing CAMHS who have SEND
- Children and young people are waiting for less time to access the support they need – measured through CAMHS wait times
- More children and young people with SEND are being well-supported in their communities, with fewer children and young people being admitted to A&E, needing crisis care or becoming a Child in Care due to a crisis related to mental health needs.
Outcomes for services
- Mental health services are more accessible for children and young people with SEND, with evidence-based, effective support offered to those with complex support needs
- Clear and effective mental health pathways are available to care-experienced children and young people – many of whom have SEND needs – and are being accessed by all those who need mental health support
- We can demonstrate that the voice of children and young people with SEND is increasingly at the heart of the ways in which mental health services are designed and delivered
- Parents, carers, families, and professionals feed back to us that outcomes have improved, that services are better meeting the individual and holistic needs of the child or young person, and that they have more trust and confidence in local services. Measured through: CHI-ESQ data (Experience of service questionnaire) and clinical outcomes data.
Children receive early and effective support to prevent a crisis. If crisis or specialist secure provision is needed, then this is provided as close to home as possible
Children and young people are best looked after and supported in safe, stable, and caring home environments. That is why we want to minimise the number of children and young people requiring emergency health and care services. This requires offering early joined-up care and support which is as close to home as possible and provided by collaborative and well-co-ordinated multi-agency teams. It also means that, where emergency care is needed by a child or young person, it is of a high-quality and supports a swift and safe return to home.
Local needs
The numbers of young people with a learning disability and/or autism admitted to an inpatient CAMHS bed have reduced from 17 at the beginning of 2020 to 4 at the end of 2020. This is a result of intensive and committed community work, to meet these young people’s needs in a community setting. Office of National Statistics would predict there to be between 2 and 3 children with autism and Learning disability in an adolescent inpatient setting at any one time given the population size in Devon. We have completed an analysis of all 14 Devon young people presenting with a ‘Bluelight’ request for admission during that period and the vast majority do not have an identifiable mental health that requires admission and treatment in a hospital setting. Many are presenting with challenging behaviour and levels of risk that make accommodation in the community difficult. However, during the winter of 20/21, we have seen a rise in the number of children with autism and learning disability entering care due to reaching crisis at home. The cause of the crisis in many cases was due to the long-term impact of the pandemic. However, in response, we are looking to offer increased support and wrap around for young people while at home through community intervention and assertive outreach as set out in earlier sections above.
The Dynamic Support Register (DSR) represents the most acute level of need within the populations of children and young people with learning disabilities and/or autism. We have been developing the use of the DSR in Devon. There are clear criteria for inclusion on the register, particularly where the young person’s needs not being met in the community, and the potential need for inpatient care as a result. The DSR therefore plays a key role in understanding needs and identifying early signs of needs that may lead to a crisis. Approximately 34 young people are currently highlighted through the DSR. We have a joint agency review underway in May and June 2021 of the children who have been identified for support through the DSR to assess unmet need and to design services and pathways to respond.
We have identified the need for a more robust community setting to support these young people without the restrictions of a hospital. It is also not appropriate to use the Mental Health Act as a legal structure to manage their care as there is no identified treatment for their presentation. These are young people who need a structured and stabilising environment, with high levels of staff support and care, to reduce their behavioural responses to trauma, chronic levels of distress and, in some cases, neglect.
Where we are now
Meeting need earlier to avoid crisis and admission to hospital
We have made significant improvements on our crisis offer to young people over the last few years, including a fully functioning and dedicated, children’s Place of Safety (POS) offer. Initially, the children’s POS was offered using the Extra Care Area of the Plymouth inpatient unit (Plymbridge House). Within the last 12 months however, a dedicated space has now been developed on the same site to support individuals requiring detention within a POS.
Effective multi-agency working, including assertive outreach delivered by CAMHS services, is supporting young people with complex needs including autism, self-harm or eating disorders to be able to remain at home with effective help and care in place. We will endeavour to build on this with the development of specialist community intervention and specialist assertive outreach for children with a range of neuro disability needs.
Emergency placements for children in care and care leavers with SEND
Providing sufficient placements that meet the individual needs and circumstances of children and young people in our care who have complex support needs is a key priority. Our principle is that children and young people are best brought up in safe, loving and fulfilling family homes. We will minimise the need for emergency same-day placements by up-skilling foster carers and staff in residential children’s homes, recruiting increased numbers of foster carers who are registered to provide placements for children with complex support needs and/or older young people in care, and develop the local market of residential children’s home placements which have specialisms in supporting children in care with AUTISM and/or learning disabilities.
Secure settings
Devon County Council commissions health services into the Atkinson Secure Childrens Home on behalf of NHSE through the mechanism of a section 10 agreement. This is good practice and allows the knowledge of commissioners of the local area, and the market, to inform service delivery models, working in partnership locally and with NHSE colleagues. Services currently delivered directly into the Atkinson are a blend of commissioned and DCC delivered services and include GP, CAMHS, Nursing service, Occupational Therapy, Speech and Language Therapy, exploitation and substance misuse services. All services work within the secure stairs framework delivering an integrated holistic offer of support to young people in order to support them to understand their health needs and feel able to manage their health and wellbeing in a positive way, thus reducing the likelihood of potential risk posed to themselves and/or others. These services further support Atkinson to help children and young people to understand manage their emotions.
What we will do
In response to the NHS Long Term Plan priorities, the needs analysis data above we have set the priorities below. We will be looking to increase feedback from children, young people, parents and carers to further inform this work through the key worker pilot.
- Ensure there is provision to meet a range of needs of young people when they are in a crisis. This includes children with autism and/or learning disabilities. We will do this by assessing options to; use the capital funding (NHSEI) has already been identified, and working jointly between the CCG, NHSEI and LAs in Devon, commission a service that can assess and stabilise young people who present in a crisis within a community setting. Options for ownership and registration of such a property and revenue funding are being explored, including dialogue with the newly formed South West Provider Collaborative[1]. This will include analysing the future of inpatient provision for young people and reviewing the options that are specifically available for young people with autism and/or learning disabilities. In addition, developing short-term supported accommodation and short breaks provision to reduce the need for residential crisis care placements.
- Adult Social Care, Children’s Services and the CCG will develop short-term crisis support for adults/young adults with complex needs, based in local communities whose escalating behaviours pose a significant risk to maintaining stability in their home environment. This will be a 3-6-month placement to prevent homelessness or care home placement, or out of county admission to ensure that the person continues to live as independently as possible.
- Expanding the number of fostering placements for children and young people with complex support needs, including children with special educational needs and disabilities particularly autism and/or learning disabilities by 50%.
- Where emergency same-day placements are needed, supporting children and young people in family-based settings. We will work with our fostering providers to secure dedicated resource for same-day placements within our external fostering market by Summer 2022. Our goal is to reduce the number of un-planned moves to children’s homes.
- Developing and embedding the Shared Lives schemes, as part of the housing pathway, to be more flexible in the range of needs that they can support, support achievement of outcomes and be part of the community.
[31] You can find out more about the forming of the South West Provider Collaborative in this blog post on the NHS website: NHS England » Bringing specialist mental health services closer to home
How we will know we are making a difference
- The timeliness and effectiveness of early interventions and prevention leads to a reduction in the escalation of needs. This will be monitored through the Dynamic Support Register and the use of CETR
- There are fewer children and young people requiring emergency residential or fostering care
- Unplanned hospital admissions for children are avoided. NHS England target is below 6 for 21/33 with current numbers at 5 which is an improvement
- Children and young people are supported to return home as soon as possible to family-based care and support and repeating crises are decreasing
- Children and young people, and their families tell us that they feel more supported to avoid a crisis, and where one occurs ensure a timely move back home.